If you often experience the sensation of “walking on a marble” or suffer from ongoing pain in the ball of your foot (forefoot), you might be dealing with a condition known as Morton’s neuroma.
While it is not a true tumor, this thickened tissue can cause varying degrees of pain or discomfort in the forefoot, potentially interfering with daily activities and physical mobility.. While it is not a true tumor, this thickened tissue can cause varying degrees of pain or discomfort in the forefoot, potentially interfering with daily activities and physical mobility.
Anatomy of the Forefoot
The forefoot, or the front portion of the foot, consists of 14 toe bones (phalanges) and five metatarsal bones that connect the forefoot to the midfoot.
The spaces between the bases of the metatarsal bones, called web spaces, are integral to the forefoot’s structure. These web spaces are categorized as follows:
- First web space: Located between the big toe and second toe.
- Second web space: Found between the second and third toes.
- Third web space: Situated between the third and fourth toes.
- Fourth web space: Positioned between the fourth and little toes.
Sensory nerves in the forefoot, known as the medial and lateral plantar nerves, run along the sole of the foot and divide into branches near the toes. These branches, called common digital plantar nerves, provide sensation to parts of the toes and traverse the web spaces.
Within each web space, the rounded ends of the metatarsal bones are connected by structures known as transverse metatarsal ligaments. These ligaments support the common digital plantar nerves as they pass underneath, playing a crucial role in foot function.
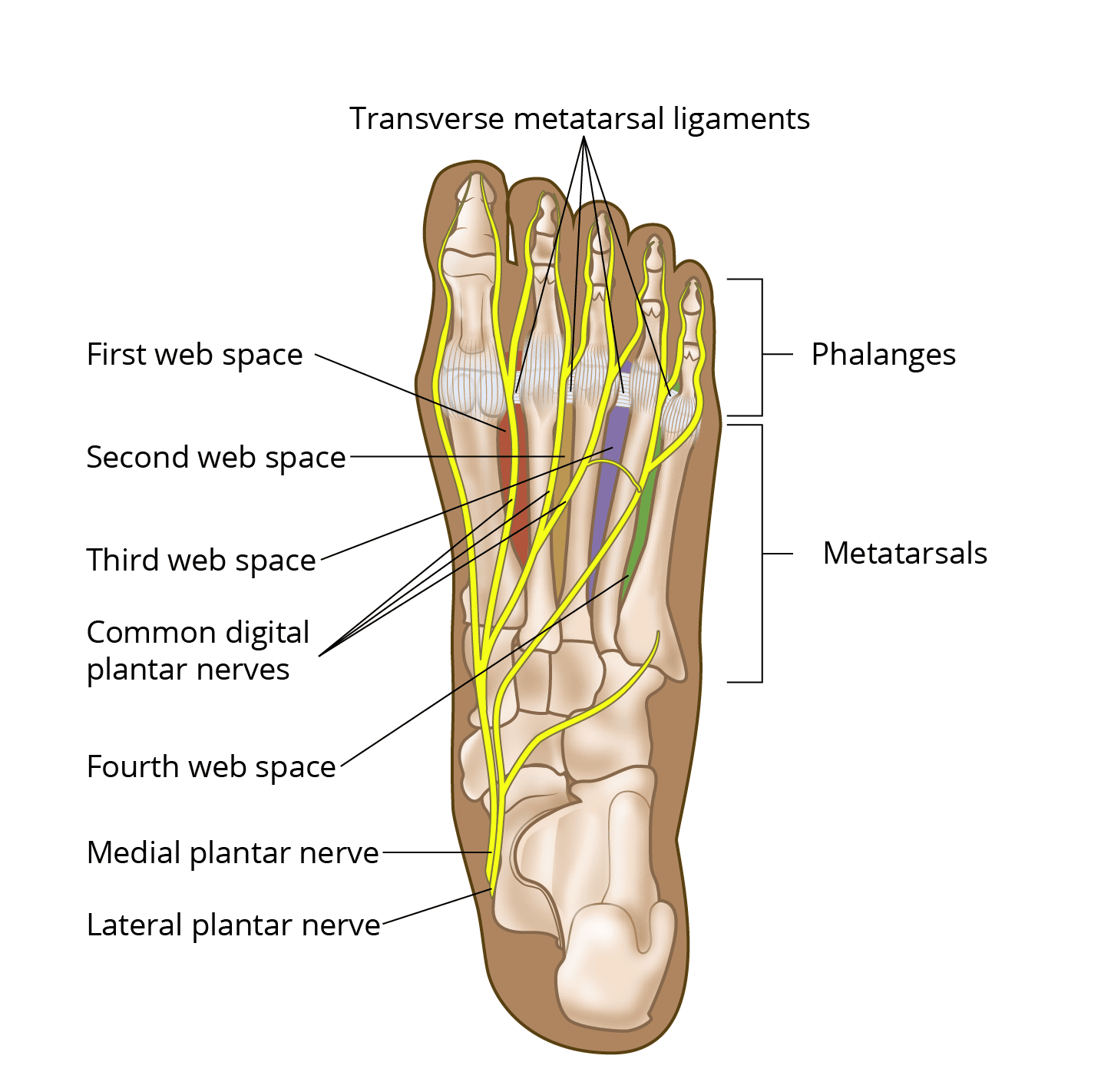 Plantar (underside) view of the foot showing the web spaces between the bases of the metatarsals, as well as the plantar nerves and transverse metatarsal ligaments.
Plantar (underside) view of the foot showing the web spaces between the bases of the metatarsals, as well as the plantar nerves and transverse metatarsal ligaments.
Description of Morton’s Neuroma
Morton’s neuroma, also known as an interdigital neuroma, Morton metatarsalgia, interdigital neuritis, or plantar neuroma, is a common condition causing pain in the forefoot.
This condition predominantly affects women, occurring approximately eight times more often in females than in males. It is most frequently diagnosed in individuals between the ages of 30 and 60, though it can appear in other age groups as well.
The neuroma usually develops in the third web space (between the third and fourth toes) due to factors like irritation, trauma, or excessive pressure. It can also occur in the second web space (between the second and third toes), albeit less commonly.
The hallmark symptom of Morton’s neuroma is pain or discomfort in the ball of the foot, located between the foot’s arches and toes on the sole. This discomfort often mimics the sensation of walking on a hard object, significantly impacting mobility and daily activities.
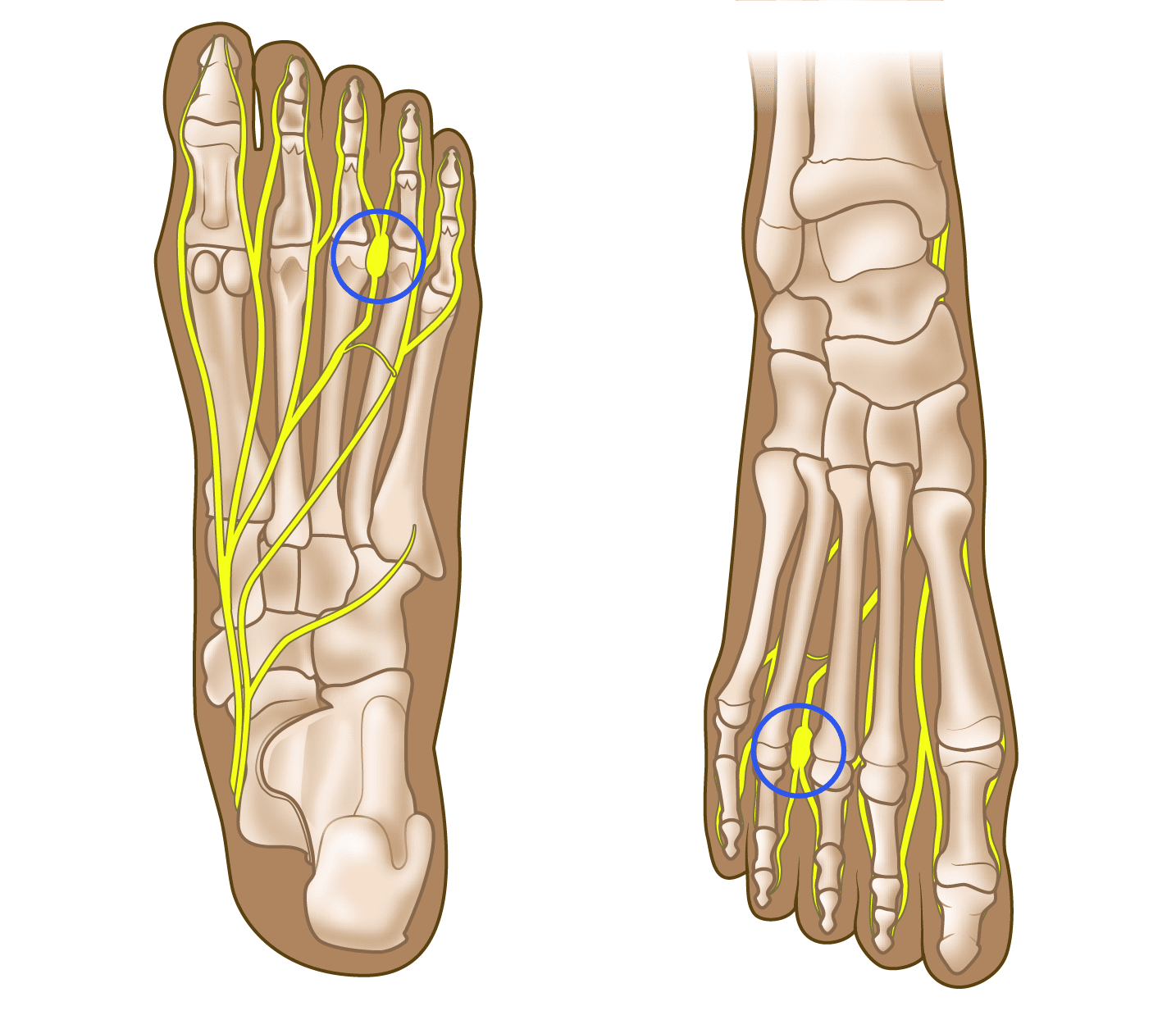 Plantar (underside) and dorsal (topside) views of the foot showing a Morton’s neuroma (circled) in the third web space.
Plantar (underside) and dorsal (topside) views of the foot showing a Morton’s neuroma (circled) in the third web space.
Cause of Morton’s Neuroma
The precise cause of Morton’s neuroma remains unclear; however, current research points to nerve entrapment as the primary factor. This condition occurs when the common digital plantar nerves in the web space experience compression or squeezing.
This repeated pressure can lead to nerve swelling and trigger the development of abnormal tissue around and within the affected nerve. Over time, this process contributes to the characteristic pain and discomfort associated with Morton’s neuroma.
Symptoms of Morton’s Neuroma
Morton’s neuroma typically does not present with visible signs, such as lumps or skin discoloration, making it a condition diagnosed primarily by its symptoms.
The most common symptoms include:
- Persistent burning or sharp pain in the ball of the foot, often radiating into the toes. This pain is most noticeable during weight-bearing activities like walking or running, while nighttime pain is uncommon.
- A sensation of stepping on a pebble or marble in the forefoot, which can be particularly bothersome when walking.
- Pain that is usually located between the base of the third and fourth toes but may also occur between the second and third toes.
- Numbness or tingling sensations in the toes, which can add to the discomfort.
- Sprinters may experience pain when pushing off from the starting block, due to the strain on the forefoot.
Footwear-related issues are a common trigger for symptoms:
- Wearing high-heeled shoes, which mimic the sprinter’s push-off position, can exacerbate the condition by increasing pressure on the forefoot.
- Tight or narrow shoes compress the metatarsal bones and pinch the nerve, worsening symptoms.
 High-heeled shoes can aggravate a Morton’s neuroma. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve
High-heeled shoes can aggravate a Morton’s neuroma. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve
When to Seek Medical Evaluation
If you experience persistent pain or discomfort in your forefoot, it is important to consult an orthopaedic surgeon for an evaluation.
Doctor Evaluation
During your visit, your doctor will assess your overall health and medical history, paying special attention to the nature, location, and severity of your symptoms. Specific questions may include:
- Which activities trigger the pain?
- What provides relief, such as rest or changing footwear?
The physical examination may involve:
- Checking the skin of the foot and ankle for pressure points.
- Evaluating the position of your toes and foot for deformities that could contribute to the pain.
- Applying pressure between the toes to locate the specific source of pain.
- Testing joint mobility to rule out conditions like arthritis or joint inflammation.
- Compressing the foot to detect a “Mulder’s click”, a sign often associated with Morton’s neuroma.
Imaging Tests
- X-rays may be performed to rule out other conditions, such as stress fractures or arthritis.
- Advanced imaging techniques, such as an MRI, may be recommended in some cases but are not always necessary.
Nonsurgical Treatment
Most cases of Morton’s neuroma can be managed with nonsurgical options, including:
- Footwear Modifications
- Avoid high heels and narrow, tight shoes.
- Opt for shoes with a wide toe box, low heels, and soft soles to reduce pressure on the nerve.
- Orthotic Devices
- Custom shoe inserts and metatarsal pads help redistribute pressure and separate the bones, relieving nerve irritation.
- Corticosteroid Injections
- These injections reduce swelling and inflammation around the nerve, often bringing significant relief.
- Some patients may benefit from nerve ablation, where medication permanently stops the nerve from transmitting pain signals.
- Alternative Therapies
- Techniques such as extracorporeal shockwave therapy and radiofrequency ablation may be considered, but their effectiveness is not yet fully proven.
Success Rates
A combination of footwear changes, orthoses, anti-inflammatory medications, and corticosteroid injections provides lasting relief for many patients.
Surgical Treatment
If nonsurgical methods fail or symptoms return, surgery may be necessary. Surgical options include:
- Nerve Removal: The affected portion of the nerve is excised.
- Tissue Release: Tight tissues surrounding the nerve are released to relieve pressure.
Procedure Details
The surgeon accesses the nerve through an incision on either the top or bottom of the foot. Afterward, they may remove the swollen section of the nerve or decompress it by releasing surrounding tissues.
Recovery
- Walking is typically allowed soon after surgery using a stiff-soled or post-op shoe.
- Avoid heavy activities and submerging the foot in water until the wounds heal, usually within 2 to 3 weeks.
- Most patients can resume wearing regular shoes about 4 weeks post-surgery.
Outcomes
- Noninvasive treatments like footwear changes and orthoses relieve symptoms in up to 50% of patients.
- Corticosteroid injections show a 50% success rate in managing symptoms.
- Advanced techniques, such as chemical or radiofrequency nerve ablation, improve symptoms for 70–80% of patients.
- Surgery has the highest success rate, with 80–95% of patients experiencing significant relief.
However, recurrence of Morton’s neuroma symptoms occurs in 5–20% of cases, requiring additional treatment. Repeat surgeries often yield similar success rates to the initial procedure.
Summary
If you have symptoms of Morton’s neuroma, consulting an orthopaedic surgeon can help determine the most effective treatment plan. While this condition can be painful, most patients achieve relief through a combination of conservative measures, injections, or surgical intervention.