Lisfranc injuries, affecting the midfoot region, occur when the bones in the midfoot are fractured or the supporting ligaments are torn. Named after the French surgeon Jacques Lisfranc de St. Martin, who first described these injuries in cavalry soldiers during the Napoleonic era, this condition remains a significant medical concern.
The severity of a Lisfranc injury can range from minor damage involving a single joint to complex cases with multiple joint disruptions and fractures. While mild Lisfranc injuries might appear similar to a simple sprain—often resulting from a straightforward twist or fall—they should not be underestimated. Damage to the Lisfranc joint is more than a routine sprain and requires careful evaluation and treatment. Left untreated, even a minor Lisfranc injury can lead to long-term complications, including chronic pain and mobility issues. Recovery often spans several months, with some cases necessitating surgical intervention for proper healing.
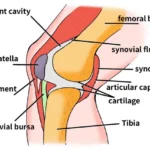
Anatomy of the Lisfranc Joint: Structure and Function
The midfoot, located in the central region of the foot, consists of a cluster of small bones that form the arch visible on the top of the foot. From this cluster, five long bones, known as metatarsals, extend outward to connect with the toes. These bones are stabilized by robust ligaments forming the Lisfranc joint complex, which secures the bones both across and along the foot. Notably, there is no ligament connecting the first and second metatarsals, making this area vulnerable to injury during twisting falls, which can result in fractures or dislocations.
The Lisfranc joint complex plays a crucial role in foot stability and function, as it permits minimal movement while providing critical support to the arch. This stability is essential for the effective transfer of force during walking, as the midfoot channels the power generated by the calf muscles toward the front of the foot. When a Lisfranc injury is not properly treated, it can lead to persistent instability in the arch, potentially causing it to collapse or flatten, which may significantly impair walking and overall foot function
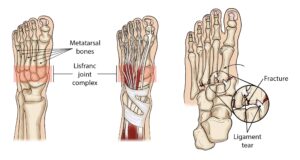 The Lisfranc joint complex includes the bones and ligaments that connect the midfoot and forefoot. Lisfranc injuries include ligament strains and tears, as well as fractures and dislocations of bone (far right).
The Lisfranc joint complex includes the bones and ligaments that connect the midfoot and forefoot. Lisfranc injuries include ligament strains and tears, as well as fractures and dislocations of bone (far right).
Description of Lisfranc Injuries
Lisfranc injuries occur when the midfoot is compromised due to fractured bones or torn ligaments. The severity of these injuries can vary significantly, ranging from a straightforward injury involving a single joint to a more complex condition that disrupts multiple joints and includes several fractures. Each type of injury requires careful diagnosis and treatment to restore proper foot function and prevent long-term complications.
 (Left) A subtle injury to the midfoot with widening between the first and second metatarsals (circle), compared with the normal foot on the left. (Center) A fracture of the second metatarsal (arrow) and a fracture of the cuboid (circle). (Right) A very severe injury of the foot from a high-energy event. It has resulted in a complete dislocation of the entire midfoot (box). Because no bones have been broken, a fusion may be recommended, given the high risk for future arthritis.
(Left) A subtle injury to the midfoot with widening between the first and second metatarsals (circle), compared with the normal foot on the left. (Center) A fracture of the second metatarsal (arrow) and a fracture of the cuboid (circle). (Right) A very severe injury of the foot from a high-energy event. It has resulted in a complete dislocation of the entire midfoot (box). Because no bones have been broken, a fusion may be recommended, given the high risk for future arthritis.
The Impact and Causes of Lisfranc Injuries
Lisfranc injuries often result in significant damage to the cartilage within the midfoot joints. This cartilage, which covers the ends of bones, facilitates smooth joint movement. When severe midfoot injuries are not treated appropriately, the damaged cartilage combined with increased stress on the joints can lead to arthritis and a collapse of the foot’s arch. Correcting such complications often necessitates complex surgical procedures. However, even with successful surgical intervention, there remains a risk of developing arthritis later in life due to the long-term effects of the injury.
Causes of Lisfranc Injuries
Low-energy Lisfranc injuries can occur from simple incidents, such as a twist and fall. These injuries are also frequently observed in athletes, particularly football and soccer players, when a player’s foot is flexed downward in a push-off position, and another player lands on the back of their foot. This mechanism of injury highlights the importance of recognizing and addressing Lisfranc injuries promptly to avoid long-term complications.
 Lisfranc injuries can occur in football or soccer when one player lands on the back of another player’s foot while the foot is flexed downward in the push-off position.
Lisfranc injuries can occur in football or soccer when one player lands on the back of another player’s foot while the foot is flexed downward in the push-off position.
Causes and Symptoms of Severe Lisfranc Injuries
Causes of High-Energy Lisfranc Injuries
Severe Lisfranc injuries are typically associated with direct trauma, such as falling from a significant height or being involved in a motor vehicle accident. These high-energy impacts often result in multiple fractures and joint dislocations within the midfoot. Additionally, such injuries may be accompanied by damage to other areas, including the back and other limbs, emphasizing the need for comprehensive medical evaluation and treatment.
Symptoms of Lisfranc Injuries
Common symptoms of a Lisfranc injury include:
- Swelling and Pain: The top of the foot may appear swollen and feel intensely painful, particularly in the midfoot region.
- Bruising: Bruising is often present on both the top and bottom of the foot. Bruising on the sole is a strong indicator of a Lisfranc injury and should not be ignored.
- Pain with Movement or Weightbearing: Pain in the midfoot tends to intensify with activities such as standing, walking, or pushing off on the injured foot. In severe cases, the pain can be debilitating, preventing weightbearing entirely and necessitating the use of crutches.
If pain and swelling persist despite standard sprain treatments such as rest, ice, and elevation, or if you are unable to bear weight on the injured foot, it is crucial to seek medical attention from an orthopedic surgeon. Prompt diagnosis and treatment are essential to prevent long-term complications and ensure optimal recovery.
 The discoloration on the bottom of the foot is very suggestive of a Lisfranc injury.
The discoloration on the bottom of the foot is very suggestive of a Lisfranc injury.
Doctor Examination: Diagnosing Lisfranc Injuries
Medical History and Physical Examination
To diagnose a Lisfranc injury, your doctor will begin by discussing your symptoms and concerns, followed by a thorough examination of your foot and ankle. While some tests may cause temporary discomfort, they will not exacerbate the injury.
During the physical examination, the doctor will look for the following key indicators:
- Bruising on the Sole of the Foot: Bruising on the bottom of the foot often signals a complete tear of the midfoot ligaments or a midfoot fracture.
- Tenderness in the Midfoot: Pain upon applying pressure to the midfoot suggests an injury to the area.
- Stress Test for Midfoot Pain: The doctor may hold your heel and twist the front of your foot to assess for pain in the midfoot. This test should not produce pain in an uninjured foot.
- Piano Key Test: By gently moving your toes up and down, the doctor applies stress across the midfoot to detect pain, a sign of potential injury.
- Single-Limb Heel Rise: You may be asked to stand on one foot and rise onto your toes. This movement puts stress on the midfoot and helps identify subtle injuries. Pain in this test indicates a problem in the midfoot.
Imaging Tests
To confirm the diagnosis, your doctor may recommend imaging tests, including:
- X-Rays: X-rays help visualize fractures and assess the alignment of the Lisfranc joint. Any misalignment may indicate ligament damage.
- Weightbearing X-Rays: If the injury is suspected to be due to a low-energy mechanism, such as a simple twist and fall, the doctor may request standing X-rays to detect subtle ligament injuries. This test does not worsen the injury or increase the likelihood of requiring surgery.
- Comparison X-Rays: X-rays of the uninjured foot may also be taken for comparison to help evaluate the alignment of the bones in the injured foot.
 (Left) In this non-weightbearing X-ray, the Lisfranc injury does not show any abnormal widening (arrow). (Right) The tear of the Lisfranc ligament is more evident in this weightbearing stress X-ray, showing a widening of the joint.
(Left) In this non-weightbearing X-ray, the Lisfranc injury does not show any abnormal widening (arrow). (Right) The tear of the Lisfranc ligament is more evident in this weightbearing stress X-ray, showing a widening of the joint.
Advanced Imaging for Lisfranc Injuries: MRI and CT Scans
Magnetic Resonance Imaging (MRI) Scan
For subtle or challenging-to-diagnose Lisfranc injuries, your doctor may recommend an MRI scan. Unlike X-rays, MRI scans excel at visualizing soft tissues, including the ligaments that are frequently damaged in a Lisfranc injury. While an MRI is not essential for diagnosing this type of injury, it can be particularly useful when the diagnosis remains uncertain or when ligament involvement needs to be confirmed.
Computerized Tomography (CT) Scan
A CT scan offers more detailed imaging than standard X-rays, producing cross-sectional and 3D images of the injured foot. This level of detail helps assess the full extent of the injury, including the number of joints affected. Orthopaedic surgeons often use CT scans to plan surgical interventions, as the detailed visualization aids in determining the best course of action. However, similar to MRI, a CT scan is not mandatory for diagnosing or treating a Lisfranc injury but serves as a valuable tool for complex cases requiring surgical planning.
Treatment Options for Lisfranc Injuries: Nonsurgical and Surgical Approaches
Nonsurgical Treatment
For mild Lisfranc injuries without fractures, dislocations, or complete ligament tears, nonsurgical treatment may suffice. This approach involves immobilization and careful monitoring:
- Immobilization: A non-weightbearing cast or boot is typically worn for 6 to 8 weeks. During this time, it is critical to avoid putting any weight on the injured foot to ensure proper healing.
- Gradual Weightbearing: After the initial immobilization phase, the patient progresses to weightbearing using a removable cast boot or a custom orthotic device.
- Regular Follow-Up: Frequent follow-up appointments with X-rays are essential to monitor the healing process. If the bones in the injured joint shift during this period, surgical intervention may become necessary to realign them.
Surgical Treatment
Surgery is typically required for more severe injuries involving displaced fractures or joint instability. The primary goal of surgical treatment is to restore the normal alignment of the midfoot and stabilize the joints for proper healing.
Two common surgical procedures for Lisfranc injuries include:
- Open Reduction Internal Fixation (ORIF):
- The surgeon makes an incision on the top of the foot, repositions the bones into their correct alignment (reduction), and secures them using plates or screws.
- As the hardware often spans joints with some natural motion, it may need to be removed 3 to 5 months after surgery, depending on the surgeon’s assessment.
- Hardware failure, such as breaking of screws or plates, can occasionally occur due to the stress of spanning mobile joints. This is not uncommon and does not typically affect the overall success of the procedure.
 Various methods of internal fixation can be used to fix Lisfranc injuries depending on the injury pattern. (Left) Multiple screws can be used. (Center) A combination of plates and screws are sometimes required when fractures are present in addition to a torn ligament. (Right) Plates that span the joints are also an excellent method of fixation.
Various methods of internal fixation can be used to fix Lisfranc injuries depending on the injury pattern. (Left) Multiple screws can be used. (Center) A combination of plates and screws are sometimes required when fractures are present in addition to a torn ligament. (Right) Plates that span the joints are also an excellent method of fixation.
Midfoot Fusion: A Surgical Option for Lisfranc Injuries
In certain cases of Lisfranc injuries, midfoot fusion may be recommended as a surgical treatment. This procedure is particularly suited for patients with severe joint damage or specific types of injuries. The goal of midfoot fusion is to realign the injured bones and allow them to heal together, effectively eliminating the joint between them. Given that the midfoot joints naturally have minimal motion, fusion is a viable solution to alleviate pain and restore functionality.
Procedure Overview
During midfoot fusion surgery:
- The surgeon removes the damaged cartilage from the affected bones.
- Metal plates, screws, or staples are used to compress the bones together, ensuring they fuse into a single, stable structure.
- Unlike other procedures, the hardware typically does not need to be removed, as the fused joints no longer require motion after healing.
 Radiographs showing a complete midfoot dislocation (left) before and (right) 2 years after fusion.
Radiographs showing a complete midfoot dislocation (left) before and (right) 2 years after fusion.
Rehabilitation and Recovery After Lisfranc Injury Surgery
Rehabilitation
Following surgery, whether Open Reduction Internal Fixation (ORIF) or midfoot fusion, a structured rehabilitation program is crucial for proper healing. The typical rehabilitation process includes:
- Non-Weightbearing Phase: Patients are required to avoid putting weight on the injured foot for 6 to 8 weeks while using a cast or cast boot. This phase allows the surgical repairs to heal without stress.
- Gradual Weightbearing: If follow-up X-rays indicate appropriate healing after 6 to 8 weeks, the patient may begin weightbearing activities while still wearing a boot. The amount of weight and the walking distance allowed are determined by the surgeon based on individual progress.
Close monitoring during rehabilitation ensures that healing proceeds as expected, and adjustments to the recovery plan may be made as needed.
Recovery
The ultimate goal for all patients is to achieve a pain-free, stable midfoot and regain full pre-injury functionality. While this is possible for many patients, recovery can vary based on the severity of the injury and individual factors:
- Timeline: Full recovery, including the resumption of all activities, may take anywhere from 6 months to 1 year.
- Challenges: Some patients may experience persistent midfoot pain, even after successful surgery.
- Athletic Performance: Athletes may face difficulties returning to their pre-injury performance levels due to the complexity of Lisfranc injuries.
- Risk of Arthritis: Despite optimal surgical outcomes, the initial cartilage damage may lead to arthritis, resulting in chronic pain. In such cases, additional surgery might be required in the future.