Radial head replacement
The procedure is performed under a combination of general and regional anaesthesia. An incision is made over the elbow’s outer aspect or back. The joint is exposed. The fragments of bone are removed. The neck of the radius is prepared and a radial head prosthesis is inserted. Any damaged ligaments are repaired. At the end of the procedure the overlying muscles are repaired and the skin is closed with sutures placed deep to the skin.
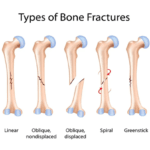
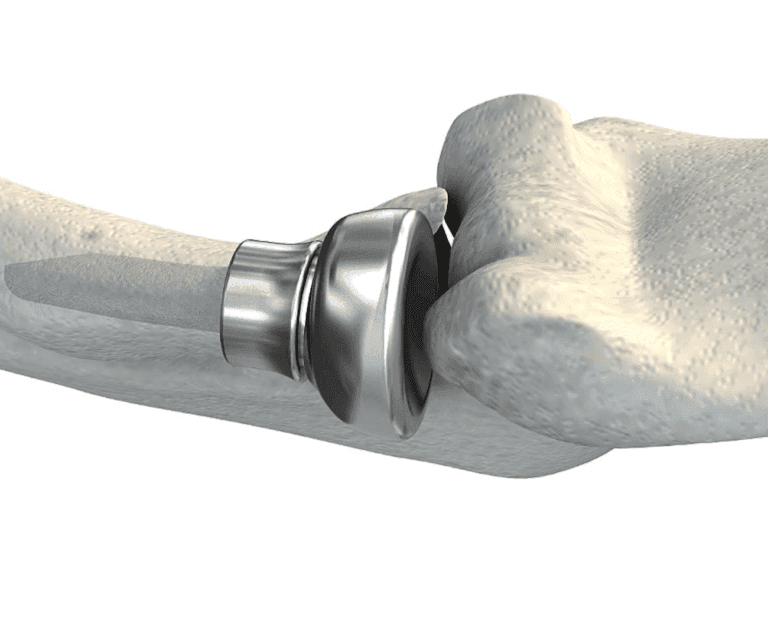
Radial head replacement surgery is undertaken on a patient’s elbow following a complex fracture to the radial head where fixation by means other than with screws or a plate is not suitable or feasible. During surgery, the fractured bone and joint surface of the radius is removed and replaced with an artificial implant. Ligament damage surrounding the elbow, commonly associated with an injured radial dial, may also be repaired during the surgery.
Following surgery, patients will have an incision on the outer aspect of their elbow. It will be sutured closed and protected by a waterproof dressing. A back-slab plaster might also be present if the associated ligament injuries were significant.


Benefits
The main benefit of the procedure is to restore stability and improve the function of the joint.
Risks
Surgical complications
Pain – The elbow may be painful for some days after surgery. This is usually managed by taking appropriate pain relieving medication and activity modification.
Bruising – Bruising may occur around the joint and the scar and usually resolves 2-3 weeks after surgery.
Bleeding – A small amount of bleeding from the surgical wound is not unusual and will usually settle after a day or two.
Numbness around the scar: A small patch of numbness adjacent to the scar is not uncommon but does not cause any functional problems.
Infection – Infection is a possibility but is rare (1%). You will be given antibiotics as a precaution.
Nerve injury – This is possible but rare.
Instability: Dislocation is a possibility. The elbow may be protected in a splint or a sling after surgery.
Stiffness: This is not uncommon following injury and surgery. In most instances it will resolve as you start moving the elbow with the aid of physiotherapy.
Heterotopic ossification: New bone may occasionally form outside the joint and impede movements, leading to stiffness. This may require surgery to remove the excess bone.
Implant related symptoms: These are uncommon. Further surgery to remove the device is rarely necessary.
Medical complications
Chest infection, Deep vein thrombosis, Pulmonary embolism, Myocardial infection are possible after surgery.
Aftercare
Following the procedure the surgical wound is covered with a shower-proof dressing. The dressing should be left undisturbed as far as possible for 14 days. If the dressing is removed for any reason it should be replaced with a similar dressing or waterproof plaster. Prior to discharge from hospital a physiotherapist will provide instructions about looking after the elbow. You will be advised to protect the elbow by wearing a sling for 4 weeks and intermittently performing movements of the elbow within certain limits. After 4 weeks you may stop wearing the sling and will be allowed to move the elbow actively through a greater range. You may resume driving at 4-6 weeks. Strengthening exercises are started after 8-10 weeks. Vigorous use of the arm or lifting heavy objects should be avoided for at least 3 months. Outpatient physiotherapy will be arranged and may need to be continued for 3-6 months.
Post-operative rehabilitation
Rehabilitation of the radial head replacement is largely dependent on the associated ligament injuries and repairs. Generally, in the case of a complex fracture, the lateral ulnar collateral ligament (LUCL) is injured necessitating surgical repair. Successful recovery is dependent on these ligaments being well protected.
Post-operatively, a patient’s arm will be in a sling and, more often-than-not, a back-slab. All dressings and bandages need to remain intact and dry until the next post-operative review. In the meantime, patients can be advised to shower using a plastic bag tied above their elbow to prevent the wound from getting wet. Alternatively, a one-handed bath can be suggested to patients at least until Kemble has reviewed the wound and assessed that it is safe to resume normal showering or bathing.
The artificial radial head should be protected at all times in order for it to integrate successfully with the bone. A patient is therefore limited to the weight-bearing of “cup of tea” for the initial six weeks. Following this period, it is recommended patients bear no more weight than 5kg on the elbow for a further six months post-operatively.
Initial Phase (0-4 weeks)
Initial appointment (10-14 days post-operatively)
- Remove post-operative dressing and primary dressing of wound
- Apply tubigrip (or similar) to elbow to reduce post-operative swelling
- Commence scar management if suitable
- Fashion posterior shell elbow splint
- splint at 120 deg of flexion to approximate radial head to coronoid process
- forearm pronation to minimise lateral stress
- wrist in neutral flexion/extension
- splint all time except for hygiene and overhead exercises exercises
- Commence overhead elbow protocol in supine position:
- shoulder flexed to 90 deg, adducted, and in neutral to slightly externally rotated position
- This position minimizes the effect of gravity, decreases posteriorly directed forces, and allows the triceps to function as an elbow stabilizer. By avoiding abduction and internal rotation, the gravitational varus force is eliminated thereby allowing the lateral collateral ligament to heal in an isometric fashion.
- With the arm in above position, following exercises are performed:
- Active assisted forearm pronation and supination, with elbow in 90 deg flexion
- Active assisted elbow flexion with no limit
- Active/active-assisted elbow extension, limited to 30 deg short of full extension
- shoulder flexed to 90 deg, adducted, and in neutral to slightly externally rotated position
- Elbow Varus Precautions (for first 6 weeks)
- avoid shoulder abduction and internal rotation
- avoid full elbow extension, especially combined with forearm supination
- when sleeping a pillow is placed between the affected arm and torso (when lying on back) or several pillows placed under elbow when side lying (on opposite side)
- if excessive pain or unexpected stiffness in motion – suggest xrays to check for subluxation of joint
Intermediate Phase (4-6 weeks post-operatively)
- Remold posterior splint to 90 deg of elbow flexion at 4 weeks, and forearm now in neutral rotation rather than pronation
- Continue supine overhead exercises as above
- Shoulder internal rotation is still avoided to minimize gravitational varus strain
Advanced Phase (6+ weeks post-operatively)
- Wean out of splint
- Start all seated range of motion exercises, capsular stretching
- Increase strength and endurance
- Commence gradual weightbearing exercises, but nothing >5kg until 6 months post surgery.
- Static progressive splinting if needed after 8 weeks
Return to activity / sports:
- The rate of healing and the readiness of a patient to return to sport or normal activities, differs from one to another. It is also highly dependent on a therapist’s input.
- Bone healing is determined via X-ray and Kemble will advise when sufficient healing as occurred for a patient to be able to return to specified activities. Most commonly, this occurs 12 weeks post operatively. However, factors such as age and general health an impact on this timeline.
- Once the bone has healed sufficiently, therapists can encourage patients to increase weight-bearing through the arm and gradually return to sports.
Signs to look for:
- Continued drainage from the wounds that does not stop after one week;
- Sudden deterioration in a patient’s pain level when previously it had been improving;
- Sudden locking of the elbow and inability to bend/straighten or rotate the forearm;
- If any of the above is noted, please contact Kemble’s team immediately.
General post-operative things to be aware of:
- It is normal to have some tingling, numbness or weakness following the procedure. This is often due to a nerve block performed pre-operatively to help with pain management or associated with a local anaesthesia which is injected postoperatively. This should wear off in a day or two.
Possible Complications:
- Early subluxation of radial head/elbow joint (posterolateral rotatory instability)
- Elbow flexion contracture (capsular tightness of anterior capsule, or posterior/lateral bony block)
- Elbow extension contracture (triceps tightness and/or posterior capsule, or anterior bony block)
- late posterolateral rotatory instability
Follow-up
An appointment will be arranged for you to be seen 2 weeks after the procedure. Follow-up may be required for at least 12 months after surgery or until a satisfactory recovery is achieved.