Background and Aims:
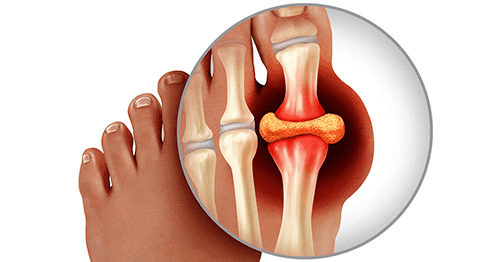
Gout is characterised by sudden, intense pain, swelling, and redness in joints or soft tissues. Initial attacks often occur in the big toe joints but can affect others. Repeated attacks may lead to inflammatory arthritis in the affected joints. Fortunately, medications can manage and treat gout attacks effectively.
Description:
Gout arises from excessive uric acid in the bloodstream, forming microscopic crystals that deposit in joints or soft tissues. These crystals disrupt smooth joint movement, causing pain and inflammation. The body treats uric acid crystals as foreign invaders, leading to an inflammatory response that resembles an infection: the affected area becomes red, swollen, hot, and tender. Acute gout attacks last 3 to 10 days, with or without treatment, but treatment accelerates symptom relief.
Affected Tissues:
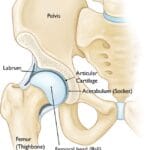
- Joints: Commonly the big toe, fingers, knees, shoulders, elbows, and hips.
- Bursae: Cushions between bones and soft tissues, notably the elbow tip (olecranon bursa) and kneecap front (prepatellar bursa).
- Tendon Sheaths: Protective tunnels for tendons in hands and feet.
- Kidneys: High uric acid levels can cause kidney stones and sometimes damage the kidneys, with 15% of gout sufferers developing kidney stones.
Progression:
After an initial attack, subsequent attacks may occur months or years later, often within two years if untreated. Later attacks might become more severe, affecting multiple joints and occurring more frequently. High uric acid levels can lead to visible, chalky deposits (tophi) around joints and tendons, causing permanent joint damage and deformity in chronic stages.
Cause:
Gout develops from excessive uric acid production or inadequate elimination, leading to hyperuricemia. Uric acid, a byproduct of purine breakdown, normally functions as an antioxidant and is excreted by the kidneys. Hyperuricemia does not always result in gout; many people with high uric acid levels do not experience gout attacks.
Risk Factors:
Gender and Age:
More common in men (ages 30-45) and post-menopausal women (ages 55-70).
Family History:
Increases risk if family members have had gout.
Medical Conditions:
High blood pressure, diabetes, kidney disease, and certain anaemias.
Medications:
Diuretics, aspirin, and cyclosporine.
Lifestyle:
Overweight, high-protein diet, excessive alcohol consumption.
Symptoms:
Gout attacks are sudden and severe. They often affect the big toe and cause red, swollen, hot, and tender joints. Fever during an attack may indicate an infection, necessitating immediate treatment. Gout is a chronic disease, and timely medical consultation is crucial for managing and preventing joint damage.
Clinical Examination:
- Blood Test: Measures uric acid levels, with high levels suggesting gout.
- Synovial Fluid Analysis: Draws fluid from inflamed joints to detect uric acid crystals and rule out bacterial infection.
Treatment:
- Acute Attack Pain Management:
- Home Remedies: Ice application, elevation, and rest.
- NSAIDs: Over-the-counter and prescription anti-inflammatory drugs.
- Colchicine: Reduces inflammation, though with potential side effects.
- Corticosteroids: Strong anti-inflammatories available in various forms.
- Nonsurgical Treatment:
- Medications: Long-term uric acid control (e.g., allopurinol, colchicine, probenecid, febuxostat) for frequent or severe attacks or presence of tophi/kidney damage.
- Lifestyle Changes: Maintain a healthy weight, hydrate, reduce calorie and fat intake, avoid sugary drinks, and limit purine-rich foods and alcohol.
- Surgical Treatment:
- Removal of Tophi: For painful or infected uric acid deposits.
- Joint Fusion: For permanent joint destruction in smaller joints.
- Joint Replacement: For end-stage arthritis in larger joints, like the knee.
Conclusion:
Proper treatment and lifestyle adjustments can manage gout and prevent its progression to disabling stages. With appropriate medical care, most people can lead everyday lives.