DEFINITION
Extensor carpi ulnaris (ECU) subluxation occurs when the separate subsheath of the sixth dorsal compartment is torn or attenuated. This results in the ECU tendon moving out of its groove in the ulna, often causing a painful click during resisted supination, ulnar deviation, and mild palmar flexion.
ANATOMY
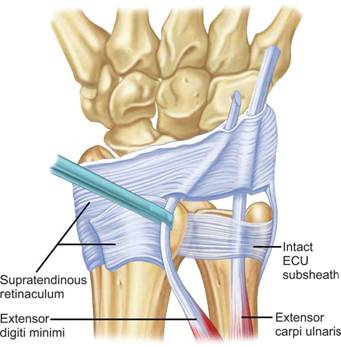
The dorsal extensor retinaculum of the wrist has two primary layers. The supratendinous retinaculum extends from the proximal to the distal radiocarpal joint, ending at the carpometacarpal joints. It forms the radial septum for the first extensor compartment and surrounds the ulna. The infratendinous retinaculum runs from the radiocarpal to the carpometacarpal joints and is found deep to the fourth and fifth extensor compartments on the radius. The ECU lies in its own separate fibro-osseous subsheath, which is a duplication of the infratendinous retinaculum and maintains the tendon in the groove.
PATHOGENESIS
Traumatic injury often involves active ECU contraction with forced supination, palmar flexion, and ulnar deviation. This is commonly reported in sports like tennis, baseball, and golf. Injuries can range from simple attenuation to complete rupture of the ECU sheath.
NATURAL HISTORY
Chronic subluxation can lead to painful snapping of the tendon with supination and pronation, progressing to ECU tendinopathy and partial tendon tears. Volar dislocation of the ECU tendon can result in distal radioulnar joint (DRUJ) instability, eventually leading to degenerative changes. In some cases, minor subluxation and related symptoms may improve with minimal intervention.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients often present with persistent ulnar wrist pain aggravated by activities requiring pronation and supination. They may feel a clicking sensation. Physical examination should focus on palpation and inspection of the sixth dorsal compartment and ECU tendon. Most acute sheath ruptures and tendinopathies will be tender to palpation at the level of the distal ulna and groove. Pain with subluxation is a critical finding when considering surgical treatment.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Routine anteroposterior (AP), lateral, and oblique radiographs in neutral rotation are important. MRI is the most sensitive imaging modality to detect ECU subluxation, often showing inflammation and partial tendon disruption. An MRI arthrogram can depict a subsheath tear and provide additional information on the TFCC and intercarpal ligaments. Ultrasound allows dynamic assessment of ECU stability and can quantify subluxation.
DIFFERENTIAL DIAGNOSIS
- ECU tenosynovitis
- TFCC injury
- Lunotriquetral ligament injury
- Ulnocarpal impaction syndrome
- Ulnar styloid nonunion
- DRUJ arthrosis
NONOPERATIVE MANAGEMENT
In the acute setting (within 3 weeks of injury), immobilize the patient in an above-elbow cast with the wrist in neutral to slight pronation, neutral to slight radial deviation, and neutral to slight extension. After 4-5 weeks, therapy is initiated, starting with a sugar-tong splint and progressing to a forearm-based splint with gradual return to activities. Unprotected full activity is allowed 3-4 months after treatment initiation.
SURGICAL MANAGEMENT
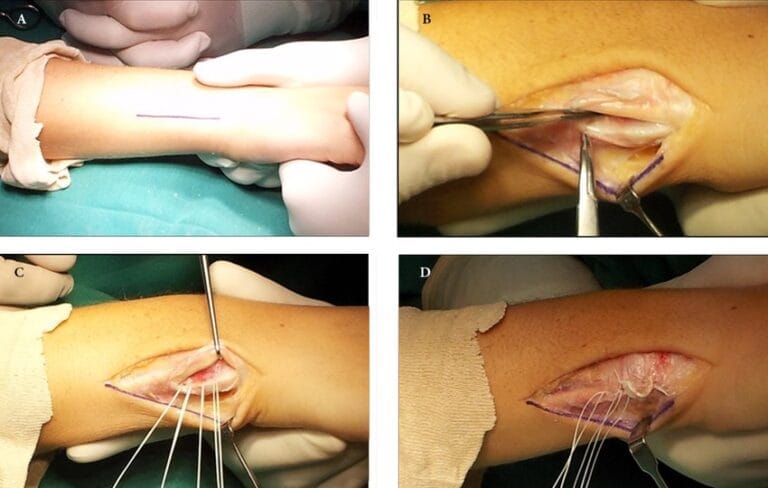
Surgical reconstruction should be considered for patients with significant symptoms related to ECU tendon subluxation, especially if the injury is more than 3 weeks old. The approach depends on the type of subsheath lesion present at the time of surgery.
Treatment of Types A and B Lesions:
- In the acute setting, suture repair may be possible and can be augmented using suture anchors.
- If the fibro-osseous sheath is ruptured and irreparable, reconstruction using a retinacular sling or free retinacular graft is preferred.
Treatment of Type C Lesions:
- Repositioning of the fibro-osseous sheath at the ulnar margin of the groove is required.
- Stretching and attenuation of the sheath without bone separation may be treated by suture imbrication, depending on tissue quality.
TABLE: Classification of Extensor Carpi UlnarisSubsheath Lesion with Recommended Surgical Treatment
| **Lesion Type | Description of Pathology | Recommended Surgical Treatment** |
| A | The fibro-osseous sheath is disrupted from the ulnar wall. The tendon may lie beneath the disrupted sheath. | If the injury is acute and adequate tissue is present, attempt direct repair. If non-reconstructible, use retinacular free graft or retinacular sling. |
| B | The fibro-osseous sheath is disrupted from the radial wall. The tendon may rest on top of the sheath and prevent healing. | A sheath reconstruction with a retinacular free graft or retinacular sling is suggested. |
| C | The fibro-osseous sheath is stripped from the periosteum but remains in coninuity, forming a false pouch. | Imbrication of the false pouch is reinforced with suture anchors or drill holes.
|