Definition
A triceps tendon rupture occurs when the tendon tears or avulses from its insertion point on the olecranon, resulting in difficulty or inability to extend the elbow against gravity or resistance. Complete ruptures involving all three heads of the triceps tendon (long, lateral, and medial) typically require surgical intervention. Partial tears may be tolerated in patients with low functional demands.
Anatomy
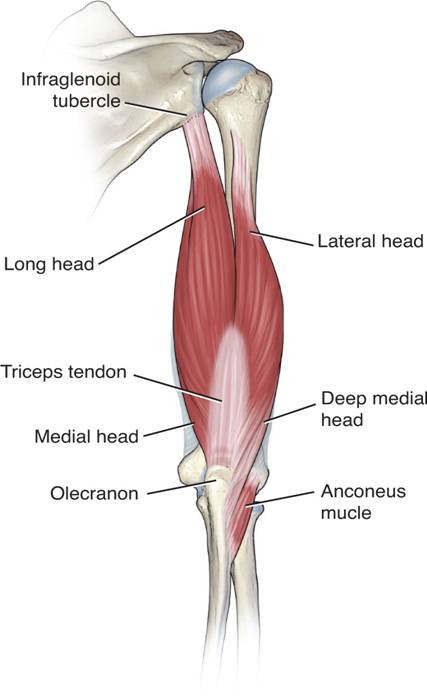
Origin The triceps brachii muscle has three heads:
- Long Head: Originates from the infraglenoid tubercle of the scapula.
- Lateral Head: Arises from the upper margin of the radial groove of the humerus.
- Medial Head: Originates below the lateral margin of the radial groove, which contains the radial nerve, covering the entire rear surface of the lower part of the humerus.
Insertion In the distal third of the posterior arm, the lateral and long heads form the superficial tendinous part of the triceps insertion on the posterior surface of the olecranon. The medial head (deep part of the triceps) inserts onto the olecranon through both muscular and tendinous fibers.
The superficial tendon has two components as it approaches the insertion area:
- Lateral Component: Expansive, relatively thin, and continuous with the anconeus muscle and fascia.
- Medial Component: Thicker than the lateral aspect, forming the proper triceps tendon that inserts directly onto the olecranon.
In some cases, a distinct interval exists between the lateral triceps expansion and the medial triceps tendon, known as triceps decussation, located along the crest of the ulna. The deep tendon is covered by thin muscle fibers medially and laterally. The deep medial head of the triceps has a broad, flat tendon centrally and laterally, while medially it is a narrow, thickened tendon.
Magnetic resonance imaging (MRI) often shows a bipartite insertion between the deep and superficial tendons of the triceps into the olecranon. All three heads of the triceps contribute to forming the dome-shaped triceps olecranon footprint.
Pathogenesis
Triceps tendon ruptures are usually caused by a sudden, forceful contraction of the triceps muscle against resistance or direct trauma to the elbow. The injury can be associated with other conditions such as olecranon bursitis or systemic diseases like rheumatoid arthritis.
Natural History
If untreated, complete ruptures can lead to significant weakness in elbow extension and functional impairment. Partial tears may heal with conservative treatment in patients with lower functional demands, but they might also lead to chronic pain and weakness if not properly managed.
Patient History and Physical Findings
Patients typically present with:
- Sudden onset of pain at the back of the elbow.
- A popping or snapping sensation at the time of injury.
- Swelling and bruising around the elbow.
- Palpable gap or defect above the olecranon.
- Difficulty or inability to extend the elbow against gravity or resistance.
Imaging and Other Diagnostic Studies
- X-Rays: May show an avulsion fracture of the olecranon.
- MRI: Useful for confirming the diagnosis, assessing the extent of the tear, and identifying any associated injuries. MRI often demonstrates a bipartite insertion between the deep and superficial components of the triceps tendon into the olecranon.
Differential Diagnosis
- Olecranon bursitis
- Distal humerus fracture
- Elbow dislocation
- Lateral epicondylitis
- Medial epicondylitis
Nonoperative Management
- Indications: Partial tears in patients with low functional demands.
- Treatment: Immobilization in a splint or brace followed by a gradual rehabilitation program focusing on restoring range of motion and strengthening the triceps muscle.
Surgical Management
Indications: Complete ruptures or partial tears in patients with high functional demands.
Procedure: Reattachment of the triceps tendon to the olecranon using suture anchors, transosseous sutures, or other fixation methods. Postoperative rehabilitation includes immobilization followed by gradual range of motion and strengthening exercises.
Postoperative Care
- Immobilization: The elbow is typically immobilized in a splint or brace for several weeks to allow for initial healing.
- Rehabilitation: Gradual range of motion exercises begin after immobilization, followed by progressive strengthening exercises to restore full function.
Outcomes
With appropriate treatment, most patients can expect to regain full strength and function in the affected arm. Early diagnosis and intervention are critical to achieving the best outcomes and preventing long-term disability.