Introduction
When the joint surfaces of the three bones in the elbow become separated, it results in an elbow dislocation. These dislocations, which can be complete or partial, typically occur following trauma, such as a fall, motor vehicle collision, or other accident. In a complete dislocation, the joint surfaces are fully separated, whereas in a partial dislocation, also known as a subluxation, the joint surfaces are only partially separated.

When an individual falls onto an outstretched arm, it can lead to the tearing of the collateral ligaments in the elbow. In cases where the tear is significant, the elbow joint may then become dislocated.
Anatomy
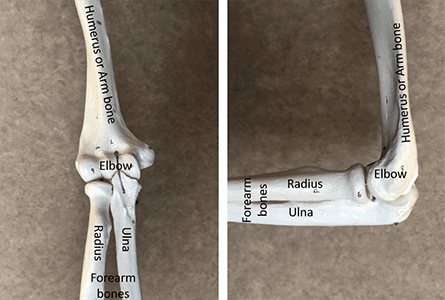
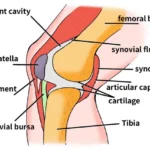
The elbow joint is formed by three bones: the humerus in the upper arm and the radius and ulna in the forearm. Each of these bones has a distinct shape, and ligaments connect them to maintain proper alignment and joint stability.
The elbow functions as a hinge joint and a ball and socket joint. Flexion and extension, which refer to bending and straightening of the elbow, occur through the hinge joint. Meanwhile, supination and pronation, involving the rotation of the hand palm up and palm down, respectively, occur through the ball and socket joint. Injuries and dislocations to the elbow can impact these motions.
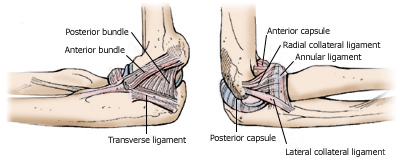
The ligaments of the elbow on the inner side (left) and outer side of the joint (right).
Cause
Elbow dislocations are relatively uncommon occurrences. Typically, they result from incidents where an individual falls onto an outstretched hand, transmitting force to the elbow with a rotational component. This mechanism is commonly observed in simple falls, motor vehicle collisions where passengers brace for impact, or in sports like wrestling or football, where rotational movements are involved.
The stability of the elbow joint relies on the combined support of bone surfaces, ligaments, and muscles. When dislocation occurs, these structures can sustain varying degrees of injury. In simple dislocations, ligament damage is predominant without significant bone involvement, while complex dislocations entail fractures alongside ligament injuries. Severe dislocations may also compromise blood vessels and nerves traversing the elbow, posing a risk of limb loss and necessitating amputation.
Risk Factors:
Your likelihood of experiencing an elbow dislocation increases if:
You have inherent laxity or looseness in your ligaments. From birth, your ulna bone has a shallow groove for the elbow hinge joint.
Symptoms:

Complete elbow dislocation
A complete elbow dislocation is highly painful and easily recognizable. The arm will appear deformed, possibly with an abnormal twist at the elbow. Symptoms of a partial dislocation (subluxation) may include:
Discomfort during elbow movement Bruising on the inner or outer side of the elbow, indicating potential ligament stretching or tearing A sensation of the elbow spontaneously shifting in and out of place abruptly and autonomously
Signs
- Snapping or cracking sensation
- Sudden, intense pain
- Swift swelling
- Complete loss of function (inability to move or utilise the elbow and hand)
- Noticeable deformity
- The elbow is slightly bent and upheld by the uninjured arm.
- Tingling and/or diminished strength in the hand and fingers
clinical Assessment
During the examination, your physician will:
Inspect your arm for tenderness, swelling, and abnormalities. Assess the skin and blood flow to the arm, including examining the pulses at the wrist. If the artery sustains injury during dislocation, the hand may feel cool to the touch and exhibit a pale or purplish coloration due to inadequate blood circulation. Evaluate the nerve function of the hand. Nerve damage from dislocation may lead to numbness and restricted movement in some or all hand parts.
Imaging Tests

An X-ray is essential to identify any bone injuries and determine the direction of the dislocation.
X-rays are the preferred method for confirming elbow dislocation.
A computed tomography (CT) scan may be ordered if bone details are unclear on X-rays. While a magnetic resonance imaging (MRI) scan can help assess ligaments, it is typically unnecessary immediately following the dislocation. The physician will proceed with elbow reduction once the dislocation is confirmed by X-ray. Any subsequent CT or MRI scans are usually performed after the elbow has been repositioned.
Treatment
Elbow dislocations demand immediate attention as they are considered emergency injuries.
Immediate Treatment aims to restore the elbow to its proper alignment, with the long-term goal of restoring arm function.
Non-Surgical
Treatment In the emergency room (ER), sedatives and pain medications are often administered before gently and slowly realigning the elbow through a reduction manoeuvre. Following successful reduction, a splint is applied to immobilise the elbow and prevent further injury. This splint remains in place until a follow-up with a physician is conducted.
Simple elbow dislocations typically involve immobilisation in a splint or sling for 1 to 3 weeks, followed by gradual introduction of range-of-motion exercises. Occupational or physical therapy may aid in regaining mobility without risking re-dislocation. Strengthening exercises may be incorporated as range-of-motion improves, with periodic X-rays taken to monitor joint alignment.
In some cases, full arm extension may not be achievable despite therapy. However, satisfactory elbow function can still be maintained.
Surgical Treatment
Persistent misalignment of the elbow joint may necessitate surgical intervention, especially in complex dislocations. Surgery aims to realign bones and stabilise severe bone injuries.
Post-surgery, the elbow is safeguarded, often with a splint or external hinge, to prevent re-dislocation.
In instances of associated blood vessel or nerve injuries, additional surgical procedures may be required to address these complications. Phisiotherapy aids in minimising stiffness during recovery, with the ultimate goal of protecting the healing elbow while mitigating scar tissue formation.
In cases where stiffness persists after healing, surgical intervention to remove scar tissue or obstacles to movement may be necessary. Although this surgery can improve elbow motion, achieving a normal range may not always be possible.
Over time, inadequate bone alignment, abnormal joint movement, or recurrent dislocations may elevate the risk of arthritis development in the elbow joint.
Research on the Horizon
Treatment for simple elbow dislocations is typically straightforward and has favourable outcomes. However, managing complex dislocations poses challenges, often resulting in some degree of permanent elbow disability. Advances in treatment are underway to enhance outcomes for these individuals.
One area of ongoing research focuses on determining the optimal timing for surgery in complex dislocation cases. Delaying surgery slightly may benefit certain patients by allowing swelling to diminish post-reduction. Following immediate reduction, a brace, splint, or external fixation frame may be employed to immobilise the elbow for approximately 1 or 2 weeks before major reconstructive surgery.
Early elbow mobilisation has shown promising results for both simple and complex dislocations. This approach helps minimise scar tissue formation and promotes improved elbow mobility. Despite challenges associated with early mobilisation in complex cases, strategies such as enhanced bone and ligament fixation techniques, improved pain management, and innovative rehabilitation methods—including continuous motion machines and dynamic splinting—can facilitate early movement and enhance overall recovery outcomes.