ShoulderPatient education
Abnormalities of the Blade
Abnormal scapula movements is a common physical sign, but because it is often asymptomatic it receives little attention. However, symptoms of pain, weakness, or cosmetic deformity may demand attentio
Published
16 July 2024
Reading time
9 min
Words
2,064
Sections
4

The scapula, or shoulder blade, is a large triangular-shaped bone that lies in the upper back. The bone is surrounded and supported by a complex system of muscles that work together to help you move your arm. If an injury or condition causes these muscles to become weak or imbalanced, it can alter the position of the scapula at rest or in motion.
An alteration (change) in scapular positioning or motion:
- Can make it difficult to move your arm, especially when performing overhead activities
- May cause your shoulder to feel weak
- Can lead to injury if the normal ball-and-socket alignment of your shoulder joint is not maintained
- The normal resting position of the scapula, or
- Normal motion of the scapula as the arm moves
Cause
Causes of scapular dyskinesis include: Weakness, imbalance, tightness, or (rarely) detachment of the muscles that control the scapula- Injuries to the nerves that supply the muscles
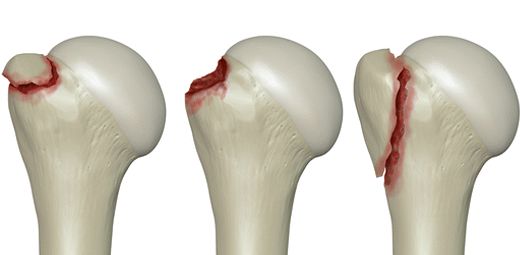
- Injuries to the bones that support the scapula or injuries within the shoulder joint
- Pain and/or tenderness around the scapula, especially on the top and medial (inner) border
- Weakness in the affected arm ' your arm may feel tired or 'dead' when you try to use it vigorously
- Fatigue with repetitive activities, especially overhead movements
- Limited range of motion ' you may be unable to raise your arm above shoulder height
- A crunching or snapping sound with shoulder movement
- Noticeable protrusion or 'winging' of the scapula
- A drooped or forward-tilted posture on the affected side
Doctor Examination
Physical Examination Your doctor will talk with you about your medical history and general health and ask about your symptoms. They will examine your entire shoulder and scapula, looking for injury, weakness, or tightness. In most cases, the physical exam will include the following: Visual observation.'Prof Imam or a member of the team will look at your affected scapula from behind, comparing it to the non-involved side. To see if scapular dyskinesis is present, your doctor may ask you to move your arms up and down 3 to 5 times, sometimes with light weights in your hands. This will usually reveal any weakness in the muscles and display abnormal motion patterns. Manual muscle testing.'Your doctor will perform strength testing of your shoulder and scapular muscles to determine if muscle weakness is contributing to the abnormal scapular motion. Corrective manoeuvres.'Specific tests involve corrective manoeuvres that will help your doctor learn more about your condition. These tests include:- Scapular assistance test (SAT).'In this test, the doctor will apply gentle pressure to your scapula to assist it upward as you elevate your arm. If your symptoms are relieved and the arc of motion is increased, it is an indication that your muscles are not strong enough to raise your arm.
- Scapular retraction test (SRT).'In this test, the doctor will test your arm strength by pushing down on your extended arm. They will then manually place the scapula in a retracted position and test your strength again. In patients with scapular dyskinesis, muscle strength will improve when the shoulder blade is retracted.
Imaging Tests
Imaging tests are not always necessary to diagnose scapular dyskinesis. Your doctor may, however, order an imaging study, such as an X-ray, computed tomography (CT) scan, or magnetic resonance imaging (MRI) scan, if they suspect a bony abnormality of the scapula (such as an'osteochondroma) or an injury to another part of the shoulder. Treatment Physiotherapy exercises will focus on strengthening and stretching the muscles around the shoulder. Nonsurgical Treatment In almost all cases, the symptoms of scapular dyskinesis will improve with nonsurgical treatment. Nonsurgical treatment may include: Nonsteroidal anti-inflammatory drugs (NSAIDs)'such as ibuprofen and naproxen, can help relieve pain and swelling. Physiotherapy.'Prof Imam'or a member of the physiotherapy team will provide an exercise program that targets the specific causes of your dyskinesis. Physiotherapy usually focuses on:- Strengthening the muscles that stabilize and move the scapula
- Stretching the tight muscles that are limiting scapular motion
SCAPULAR WINGING'
Scapula Winging The shoulder blade is the largest bone of the shoulder complex and has the greatest number of'muscles'attached to it. These muscles both stabilise the arm to the body and move the arm around in space. All these muscles act at the same time sometimes and oppose each other at other times, but work together like a well-trained team to allow the arm to move in space. If any of these muscles are not working in the right way at the right time this leads to a break in the rhythmic motion of the scapula. This is known as a scapula ''dysrhythmia''. This leads to the apparent 'winging' of the scapula. Causes: 1. Loss of serratus anterior muscle function When one talks about winging of the scapula, true winging is due to serratus anterior muscle dysfunction. This is an uncommon condition and may arise from traumatic injury to the nerve supplying the serratus anterior muscle, the long thoracic nerve; or due to damage to the nerve from pressure lesions or a neuritis (inflammation of the nerve). The long thoracic nerve follows a long an tortuous course from the neck to the serratus anterior muscle. It is prone to injury as it is much more vulnerable than many of the other nerves of the brachial plexus. The test for identifying a long thoracic nerve injury is the 'serratus wall test'. The patient is asked to face a wall, standing about two feet from the wall and then push against the wall with flat palms at waist level. Nerve conduction studies and EMG tests of the long thoracic nerve, serratus anterior muscle and other muscles of the shoulder blade are beneficial to diagnose and quantify the degree of nerve and muscle damage. The tests are also useful to assess and follow the recovery of the nerve. The treatment will depend on the cause and severity of the injury. Exploration and decompression of the nerve can be performed, where it gets trapped or damaged at the scalene muscles in the neck. For more advanced cases, the Pectoralis muscle can be performed. 2. Loss of trapezius muscle function The trapezius muscle is a large muscle above your scapula which lifts and rotates your scapula. It is the muscle you use to shrug your shoulders. Isolated loss of trapezius function is extremely rare and may occur after radical neck surgery (for tumours), where the nerve supplying the trapezius may be damaged (the spinal accessory nerve). Many people can manage with loss of trapezius function, but some have weakness and difficulty with manual and overhead activities. If the diagnosis is made early, then surgical reconstruction of within 20 months of the injury the nerve or nerve release (neurolysis) should be considered 3. Weakness of all the scapula stabilisers Muscular dystrophies, most commonly'facioscapulohumeral'dystrophy''(FSHD), are the main cause of the weakness of all the scapula stabilising muscles. 4. Loss of scapular suspensory mechanism The'coracoclavicular ligaments'suspend the scapula from the clavicle and the'acromioclavicular joint'is the only joint linking the scapula to the rest of the body. Therefore Acromioclavicular joint dislocation or fracture of the outer third of the clavicle, with rupture of the coracoclavicular ligaments, leads to an abnormal scapula rhythm and apparent scapula winging with overhead manoeuvers. This is usually not painful and usually only affects overhead workers and athletes. Another rare cause is the 'scapulothoracic dissociation', described by Rockwood & Matsen in 1990. The scapula is wrenched from the body in violent trauma leading to fracture of the clavicle and soft tissues around the clavicle. 5. Winging of the scapula secondary to instability This is one of the commonest causes of'scapula dysrhythmias'(and winging).'Recurrent dislocations of the shoulder'lead'to dysfunction of the muscles that move and support the shoulder complex and scapula. The more frequent the dislocations and the less trauma involved in causing the dislocations, the worse the scapula dysrhythmia (winging). An essential part of treating shoulder instability (recurrent dislocations) is treating scapula dysrhythmia. This is done by an'experienced physiotherapist'in association with a shoulder surgeon. 6. Winging secondary to pain This is another common cause of secondary winging and dysrhythmia of the scapula. Any painful condition of the shoulder will lead to abnormal movements of the entire shoulder complex. Reduced movement at the glenohumeral joint will lead to more compensatory movement at the scapula. 7. Brachial Plexus injury or disease Most of the nerves supplying the stabilising muscles of the scapula arise from the Brachial Plexus. The Brachial Plexus is a bundle of nerves running from the neck to the arm. It carries the nerve supply for the muscles of the arm and shoulder. Sometimes a major accident can affect the muscles of the shoulder more than the arm and lead to winging. When there is no trauma, a condition known as'Parsonage-Turner syndrome'(Brachial Neuritis) can lead to weakness of the scapula muscles.Keep reading