

A rupture in the biceps tendon at the shoulder may result in weakened arm strength and discomfort, particularly when rotating your arm from palm down to palm up.
While many individuals can manage well with this injury using simple treatments, surgery may be necessary if symptoms persist despite nonsurgical options, muscle cramping or pain develops, or full strength recovery is needed.
Anatomy

Your shoulder operates as a ball-and-socket joint comprised of three bones: the upper arm bone (humerus), shoulder blade (scapula), and collarbone (clavicle).
Within this structure, the head of the upper arm bone fits into a rounded socket located in the shoulder blade, known as the glenoid.
A complex network of muscles and tendons, collectively referred to as the rotator cuff, is present to maintain proper alignment of the arm bone within the socket.
These structures surround the head of the upper arm bone and establish connections with the shoulder blade.
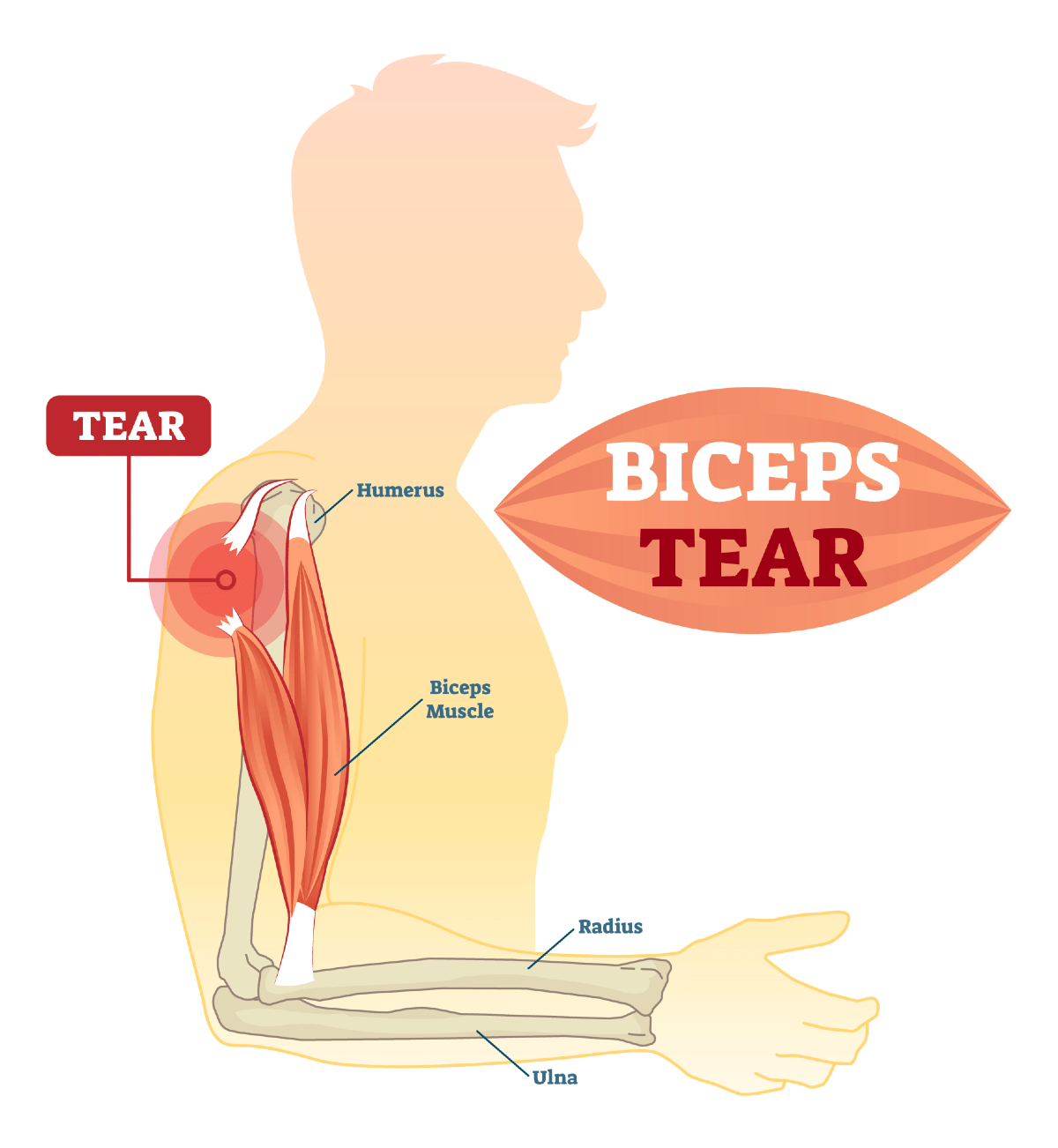
Towards the upper end of the biceps muscle, two tendons link it to bones within the shoulder. Specifically, the long head attaches to the top of the shoulder socket (glenoid), while the short head connects to a projection on the shoulder blade, known as the coracoid process.
Understanding Biceps Tendon Tears
Biceps tendon tears can occur in partial or complete forms.
Partial tears: Many tears do not fully sever the tendon.
Complete tears: A complete tear will divide the tendon into two pieces.
In numerous instances, torn tendons start with fraying and progress to complete tears, especially when lifting heavy objects.
The long head of the biceps tendon is more susceptible to injury due to its vulnerable passage through the shoulder joint to its attachment point in the socket.
Fortunately, the biceps possess two attachments at the shoulder, with the short head rarely experiencing tears.
This secondary attachment allows most individuals to utilise their biceps even after a complete tear of the long head.
Tearing the biceps tendon can damage other shoulder components, such as the rotator cuff tendons.
Causes and Risk Factors
Biceps tendon tears typically stem from two primary causes: injury and overuse.
Injury:
Tearing of the biceps tendon can occur from falling hard on an outstretched arm and lifting objects beyond one’s capacity.
Overuse:
Many tears result from gradual wear and tear of the tendon over time, which naturally advances with age and can be exacerbated by repetitive shoulder movements.
Overuse activities, such as repetitive overhead sports like swimming or tennis, can lead to shoulder issues, including tendinitis, impingement, and rotator cuff injuries. These conditions can increase stress on the biceps tendon, heightening the risk of weakening or tearing.
Risk Factors:
- Age: Older individuals are more prone to tendon tears due to accumulated wear and tear.
- Heavy Overhead Activities: Engaging in activities that involve heavy overhead lifting can accelerate tendon degeneration.
- Shoulder Overuse: Repetitive overhead sports and activities can contribute to tendon wear and tear.
- Smoking: Nicotine use can impact tendon nutrition, potentially increasing susceptibility to tears.
- Corticosteroid Medications: The usage of corticosteroids has been associated with heightened muscle and tendon weakness.
Symptoms of a biceps tendon tear include:
- Sudden, sharp pain in the upper arm.
- Audible pop or snap.
- Biceps muscle cramping with strenuous arm use.
- Bruising from the upper arm to the elbow.
- Pain or tenderness at the shoulder and elbow.
- Weakness in the shoulder and elbow.
- Difficulty rotating the hand palm up or down.
- The appearance of a bulge in the upper arm (“Popeye Muscle”) due to the tendon’s inability to keep the muscle tight.
Clinical Examination
Upon evaluation, your doctor will conduct a thorough medical history review and physiotherapy examination.
Complete ruptures are often evident due to noticeable arm muscle deformities (“Popeye Muscle”).
Partial tears may require specific manoeuvres to diagnose, such as bending the arm and tightening the biceps muscle to assess pain. Additionally, your doctor will check for associated shoulder issues and may order further tests to identify any additional problems.
Imaging Studies
X-rays:
While X-rays don’t reveal soft tissues like the biceps tendon, they are valuable in excluding other shoulder and elbow discomfort sources.
Magnetic Resonance Imaging (MRI):
Compared to X-rays, MRI scans offer superior visualisation of soft tissues. They are effective in detecting both partial and complete tears.
Treatment Options
Nonsurgical Approach
For many individuals, discomfort associated with a long head of the biceps tendon tear typically diminishes over time, and mild arm weakness or deformity may not significantly impact daily activities.
Moreover, nonsurgical interventions are often considered f no critical structures, such as the rotator cuff, are affected, These may entail:
Ice:
Applying cold packs for 20-minute intervals several times a day helps reduce swelling. It’s essential to avoid direct skin contact with ice.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs):
Medications like ibuprofen, aspirin, or naproxen can alleviate pain and swelling.
Rest:
Limiting heavy lifting and overhead activities can alleviate pain and reduce swelling. Your doctor might recommend using a sling for a brief period.
physiotherapy:
Engaging in flexibility and strengthening exercises aids in restoring shoulder movement and strength.
Surgical Intervention
Surgery is seldom required for a long head of the biceps tendon tear. However, individuals experiencing muscle cramping and persistent pain or those requiring full recovery of strength (such as athletes or manual labourers) may benefit from surgery.
Additionally, surgery might be considered for individuals with partial tears who do not find relief with nonsurgical methods.
Procedure:
Various minimally invasive procedures have been developed to repair the tendon by re-anchoring it back to the bone. Your doctor will discuss the most suitable options for your specific case.
Complications:
Complications associated with this surgery are uncommon, with re-rupture of the repaired tendon being rare.
Rehabilitation:
Following surgery, a sling may temporarily immobilise your shoulder. Rehabilitation typically begins soon after, involving therapeutic exercises to enhance shoulder flexibility and gradually incorporating strength-building exercises into your recovery plan.
Adhere to your doctor’s treatment regimen. Although rehabilitation is a gradual process, your dedication to physiotherapy will significantly influence your ability to eventually resume all desired activities.
Surgical Outcome:
Successful surgery aims to correct muscle deformity and restore nearly normal strength and function to your arm.



