Pilon fractures are a distinct type of injury affecting the lower end of the tibia (shinbone), specifically involving the weight-bearing surface of the ankle joint. These fractures often extend to the fibula, the other bone in the lower leg. Typically resulting from high-impact incidents such as motor vehicle accidents or falls from significant heights, pilon fractures are considered severe and can have lasting effects on ankle function.
The term “pilon” originates from the French word for “pestle,” symbolizing the crushing or splitting nature of the bone often seen in these injuries. Due to the high-energy trauma, the tibia may fracture into multiple fragments or be extensively crushed.
In most cases, surgical intervention is required to realign the bone and restore its structure. Because the force required to cause a pilon fracture is substantial, patients often sustain additional injuries that may also necessitate medical attention
Anatomy of the Ankle Joint
The lower leg consists of two primary bones:
- Tibia: Commonly referred to as the shinbone, it is the larger and more prominent bone of the lower leg.
- Fibula: A slender, smaller bone that runs parallel to the tibia.
At the ankle joint, these bones connect with the talus, a small yet critical bone in the foot that functions as a hinge. Together, the tibia, fibula, and talus form the structure of the ankle joint, enabling stability and movement.
This structure is integral to the ankle’s ability to support weight and provide mobility, emphasizing its importance in overall lower limb function.
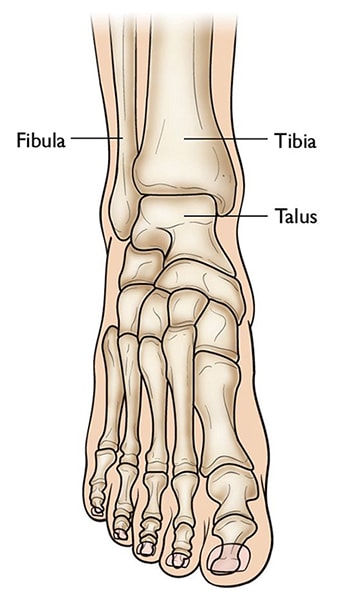 The three bones that come together to form the ankle joint.
The three bones that come together to form the ankle joint.
Understanding the Severity of Pilon Fractures
Pilon fractures can vary significantly in their complexity. The tibia may sustain a single break or be shattered into multiple fragments.
The severity of a pilon fracture is influenced by several key factors:
- Number of Fractures: The extent to which the bone is fractured.
- Bone Fragmentation: The size and quantity of the broken pieces.
- Displacement: The alignment of the fractured pieces. In less severe cases, the bone fragments may remain closely aligned. In more complex fractures, significant gaps or overlapping of the fragments may occur.
- Soft Tissue Damage: Injuries to nearby muscles, tendons, and skin often accompany the fracture.
When a fracture causes bone fragments to pierce the skin or creates an open wound that exposes the bone, it is classified as an “open” or compound fracture. This type of fracture is particularly dangerous due to the increased risk of infection in the bone and surrounding tissue. Immediate medical intervention is critical to minimize the likelihood of infection and ensure proper healing.
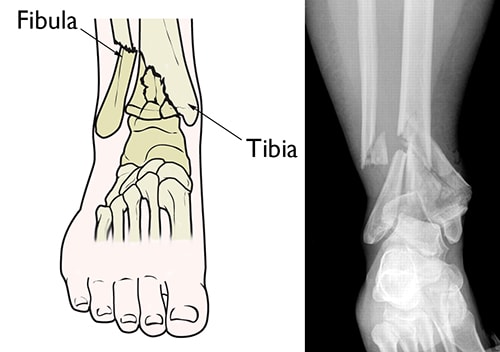 (Left) A pilon fracture often affects both bones of the lower leg. (Right) In this x-ray, both the tibia and fibula are fractured and the pieces of bone are severely displaced.
(Left) A pilon fracture often affects both bones of the lower leg. (Right) In this x-ray, both the tibia and fibula are fractured and the pieces of bone are severely displaced.
Causes of Pilon Fractures
Pilon fractures are most commonly caused by high-energy trauma. Typical scenarios include motor vehicle or motorcycle accidents, falls from significant heights, or skiing incidents.
The increased prevalence of pilon fractures correlates with the widespread use of airbags in modern vehicles. While airbags significantly improve survival rates in high-speed collisions, they do not provide protection to the legs, leaving survivors susceptible to severe lower limb injuries, including pilon fractures.
Symptoms of Pilon Fractures
Pilon fractures are characterized by immediate and intense pain. Additional symptoms may include:
- Swelling
- Bruising
- Tenderness in the affected area
- Difficulty or inability to bear weight on the injured leg
- Visible deformity, where the ankle may appear misaligned or crooked
Doctor Examination and Initial Stabilization
Pilon fractures typically necessitate emergency care due to the severe symptoms and the potential for associated injuries. Patients often present to urgent care or emergency departments following high-energy trauma.
In many cases, these individuals may also sustain additional injuries to other areas such as the head, chest, abdomen, or limbs. Significant blood loss from such injuries can result in shock, a potentially fatal condition that can lead to organ failure.
Physical Examination
During the evaluation, your doctor will:
- Inspect the lower leg and ankle for visible injuries, such as cuts or wounds, and gently apply pressure to identify tender spots.
- Assess toe movement and sensation throughout the foot to rule out nerve damage.
- Check pulses at critical points in the foot to ensure proper blood flow.
- Evaluate the degree of swelling in the foot and ankle, which will help determine the timing of any surgical intervention.
- Conduct a thorough examination of the rest of the body to identify any additional injuries. It is crucial to inform your doctor about any other areas of pain or discomfort.
Imaging Tests for Diagnosis
Imaging studies play a vital role in diagnosing pilon fractures and planning treatment, particularly if surgery is required.
- X-rays: These provide detailed images of the bones and are used to identify fractures or joint misalignments in the leg, ankle, and foot.
- Computed Tomography (CT) Scans: CT scans offer more precise information about the fracture’s complexity, showing detailed fracture lines and aiding in surgical planning. A CT scan may be performed immediately or after the application of an external fixator, depending on the treatment timeline.
 To fully evaluate your fracture, your doctor may recommend an x-ray (left), a CT scan (center), or a three-dimensional CT scan (right).
To fully evaluate your fracture, your doctor may recommend an x-ray (left), a CT scan (center), or a three-dimensional CT scan (right).
Treatment Options for Pilon Fractures
Most pilon fractures require surgical intervention, but in some rare cases, nonsurgical treatment may be sufficient. The decision depends on the stability of the fracture and the degree of displacement of the bone fragments.
Nonsurgical Treatment
Nonsurgical management may be suitable for:
- Stable fractures with little to no displacement of the bone fragments.
- Patients who are unable to walk or have severe medical conditions that make surgery too risky.
Nonsurgical Treatment Methods
- Splints and Casts:
Initially, a splint is applied to stabilize the ankle. Once the swelling subsides, it is replaced with a short leg cast. Proper fit is crucial, and frequent cast changes may be necessary as swelling decreases to maintain support. - Monitoring Progress:
Regular follow-up appointments, including X-rays, are essential to ensure the fracture remains stable throughout the healing process. - Recovery Process:
- Patients typically cannot bear weight on the injured ankle for up to 12 weeks.
- Mobility aids like crutches or a walker may be recommended.
- After six weeks, the cast may be replaced with a removable brace to protect the ankle as it continues to heal.
Surgical Treatment
Surgery is often required for unstable fractures where the bones are misaligned or displaced.
Open Reduction and Internal Fixation (ORIF)
This surgical technique involves:
- Repositioning (reducing) the displaced bone fragments to their normal alignment.
- Securing the fragments using screws and metal plates attached to the bone’s outer surface.
Timing of Surgery
Surgery may be delayed if significant swelling or blisters are present, as performing surgery prematurely increases the risk of infection or complications at the incision site.
- Swelling typically takes up to two weeks or more to subside.
- During this time, the ankle may be stabilized with a splint or external fixator, and in some cases, a smaller initial surgery may be performed to prepare for the definitive procedure.
External Fixation
An external fixator may be used to stabilize the fracture and maintain proper alignment while waiting for the main surgery. This temporary device holds the bones in place externally to protect the ankle during the interim period.
 An external fixator may be applied to protect your foot until it is safe to perform a second surgery to repair the fracture.
An external fixator may be applied to protect your foot until it is safe to perform a second surgery to repair the fracture.
External Fixation and Surgical Management for Pilon Fractures
In some cases, an external fixator is used as part of the surgical process to stabilize a pilon fracture. During this procedure, small incisions are made in the skin, and metal pins are inserted through the bones. These pins extend outward and are connected to carbon fiber bars positioned outside the skin, forming a supportive frame. This device helps maintain proper alignment of the ankle, restores limb length, and provides stability until a secondary surgery can be performed.
Secondary Surgery
Once swelling and blisters from the initial injury have subsided, the second stage of surgery is conducted. During this procedure:
- Bone Realignment: The displaced fragments are carefully repositioned (reduced) to restore their normal alignment.
- Internal Fixation: The repositioned fragments are secured using metal plates and screws.
- Removal of External Fixator: After the plates and screws are in place, the external fixator is typically removed.
Additional Considerations for Complex Fractures
- Fibular Fractures: If the fibula is also fractured, your doctor may first repair the fibula to stabilize the ankle before applying an external fixator. This ensures the tibia and fibula are correctly aligned. The tibia is then addressed in a subsequent procedure using metal plates and screws after swelling has decreased.
- Severe Soft Tissue and Bone Damage: In cases where the skin and bone are significantly compromised, large surgical incisions may pose a high risk of infection or further injury to the tissue. To minimize this risk, the fracture may be treated with an external fixator alone or combined with selective use of screws.
 Plates and screws may be used to fix the break, as long as the skin and surrounding tissues are healthy.
Plates and screws may be used to fix the break, as long as the skin and surrounding tissues are healthy.
Pain Management
Pain is a natural part of the recovery process following surgery. To help you heal more comfortably and effectively, your medical team will provide strategies to reduce pain.
Short-term pain relief is often achieved with a combination of medications, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. This multimodal approach minimizes reliance on opioids, reducing the risk of addiction. However, opioids must be used cautiously and only as prescribed. If pain persists beyond a few days, consult your doctor for guidance.
Early Recovery
Recovery begins gradually, often with ankle movement starting 2 to 6 weeks after surgery. The timing depends on your specific fracture, treatment approach, and whether an external fixator is used. External fixators may delay movement until they are removed.
To prevent blood clots during immobilization, doctors frequently prescribe blood thinners during the early stages of recovery.
Weight-Bearing Restrictions
Most patients are unable to bear full weight on the injured ankle for 2 to 3 months. During this time, crutches, a cane, or a walker will be necessary to aid mobility.
Physical Therapy and Rehabilitation
Once movement is permitted, a removable cast or brace may be provided to facilitate physical therapy. Early exercises focus on improving ankle range of motion, while muscle-strengthening exercises are typically introduced around six weeks after surgery.
By four months post-surgery, many patients no longer require braces or walking aids. However, continued exercises are crucial, as ankle function may improve for up to two years after injury.
Common Complications After Pilon Fractures
- Infection:
Delayed surgery reduces the risk of infection, now affecting less than 10% of patients. Minor infections are managed with antibiotics, while severe infections may require intravenous treatment or, in rare cases, surgery. - Stiffness:
Ankle stiffness is common, and full pre-injury mobility may not be regained. Tasks like climbing stairs or ladders may remain challenging. - Post-Traumatic Arthritis:
About half of pilon fracture patients develop arthritis due to cartilage damage, leading to pain and stiffness over time. Treatment may involve further surgery or symptom management. - Bone Healing Issues:
If the fracture does not heal properly, additional surgery may be required, often involving a bone graft from your body (autograft) or a donor (allograft), along with plates or screws. - Other Complications:
- Discomfort from plates or screws (these can be removed after healing).
- Wound healing problems.
- Blood vessel or nerve damage caused by the injury or surgery.
Outcomes and Long-Term Recovery
Recovery depends on the severity of the fracture, your overall health, and the nature of your activities.
- Patients with sedentary jobs may resume work sooner, while those with physically demanding jobs often need 4 to 6 months of rehabilitation.
- High-impact sports may be resumed six months after surgery, though stiffness, discomfort, and limping may persist for several months.
Your symptoms and mobility typically continue to improve for up to two years post-injury, and your doctor or physical therapist will help you regain function progressively.
Questions to Discuss With Your Orthopaedic Surgeon
To ensure clarity about your treatment and recovery, consider asking your doctor:
- When can I start putting weight on my leg?
- How long will I be unable to work?
- Do I have specific risks that might affect my recovery?
- What are the benefits and risks of surgery?
- Are my bones weak?
- Will I develop arthritis or other long-term complications?