Lateral collateral ligament (LCL) reconstruction is a surgical procedure aimed at repairing or reconstructing the LCL complex of the elbow. This ligament is crucial for maintaining elbow stability, particularly in preventing posterolateral rotatory instability (PLRI). LCL injuries often occur after significant elbow trauma, such as a dislocation.
Why is LCL Reconstruction Needed?
LCL injuries can result from severe elbow trauma, multiple surgeries to the lateral side of the elbow, or even corticosteroid injections. These injuries may lead to PLRI, which is a type of elbow instability that can cause the elbow joint to become unstable and dislocate.
Understanding the LCL Complex
Anatomy of the LCL
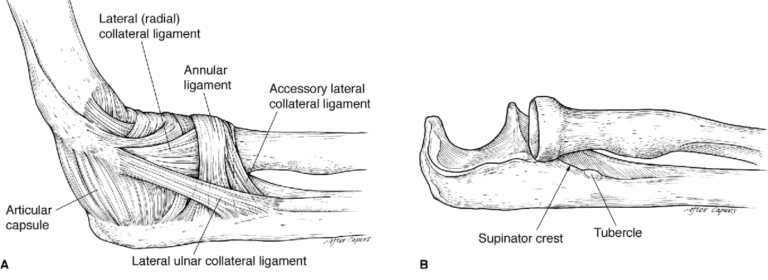
The LCL complex consists of four major components:
- Lateral Ulnar Collateral Ligament (LUCL), also known as the Radial Ulnohumeral Ligament (RUHL)
- Radial Collateral Ligament (RCL)
- Annular Ligament
- Accessory Collateral Ligament
Function of the LCL Components
- LUCL: The most critical stabilizer against PLRI, attaching to the supinator crest of the ulna.
- RCL: Resists varus stress, providing anterior stability.
- Annular Ligament: Wraps around the radial head and neck, stabilizing the proximal radioulnar joint (PRUJ).
- Capsule: Acts as a static stabilizer, especially in the extended arm.
- Muscles: The anconeus and extensor muscle groups serve as dynamic stabilizers.
Causes of LCL Injuries
LCL injuries typically result from:
- Trauma: Such as falls or direct blows that lead to elbow dislocation.
- Multiple Surgeries: Repeated procedures on the lateral side of the elbow can weaken the LCL.
- Corticosteroid Injections: These can lead to ligament attenuation, reducing recovery rates.
- Cubitus Varus: Residual misalignment after supracondylar humerus fractures can cause LCL attenuation.
How LCL Injuries Lead to Instability
- PLRI: Injury to the LCL can cause PLRI, where the ulnohumeral joint rotates and the radial head dislocates posteriorly.
- Mechanism: When the forearm is supinated and slightly flexed, a valgus stress can cause the ulnohumeral joint to rotate, leading to compression of the radiocapitellar joint and potential dislocation.
Patient Symptoms and Diagnosis
History and Symptoms
Patients may report:
- Trauma: A significant injury event.
- Recurrent Lateral Epicondylitis: Persistent lateral elbow pain.
- Previous Surgery: History of surgical interventions on the elbow.
Physical Examination
- Pain and Instability: Examination may reveal pain, instability, and reduced range of motion.
- Older Patients: May not show full dislocation but can have instability symptoms.
Treatment and Surgical Approach
Indications for Surgery
LCL reconstruction is considered when:
- Significant Instability: Due to severe trauma or multiple previous interventions.
- Persistent Symptoms: Non-surgical treatments have failed to relieve symptoms.
Surgical Procedure
The surgery involves:
- Incision and Exposure: Carefully exposing the LCL complex.
- Reconstruction: Using grafts or other techniques to restore the LCL structure.
- Protection of Nerves: Ensuring the posterior interosseous nerve and other structures are protected during the procedure.
Recovery and Rehabilitation
Postoperative Care
- Immobilization: Initial period of immobilization to allow healing.
- Physical Therapy: Gradual reintroduction of movement to regain strength and stability.
Expected Outcomes
- Improved Stability: Significant reduction in elbow instability and improved function.
- Recovery Time: Varies based on the extent of the injury and surgical technique used.
Conclusion
Lateral collateral ligament reconstruction is a critical procedure for restoring elbow stability in patients with significant LCL injuries. Proper diagnosis, surgical intervention, and postoperative care are essential for achieving the best outcomes and returning to normal activities. Always follow your doctor’s advice and attend follow-up appointments to ensure optimal recovery.
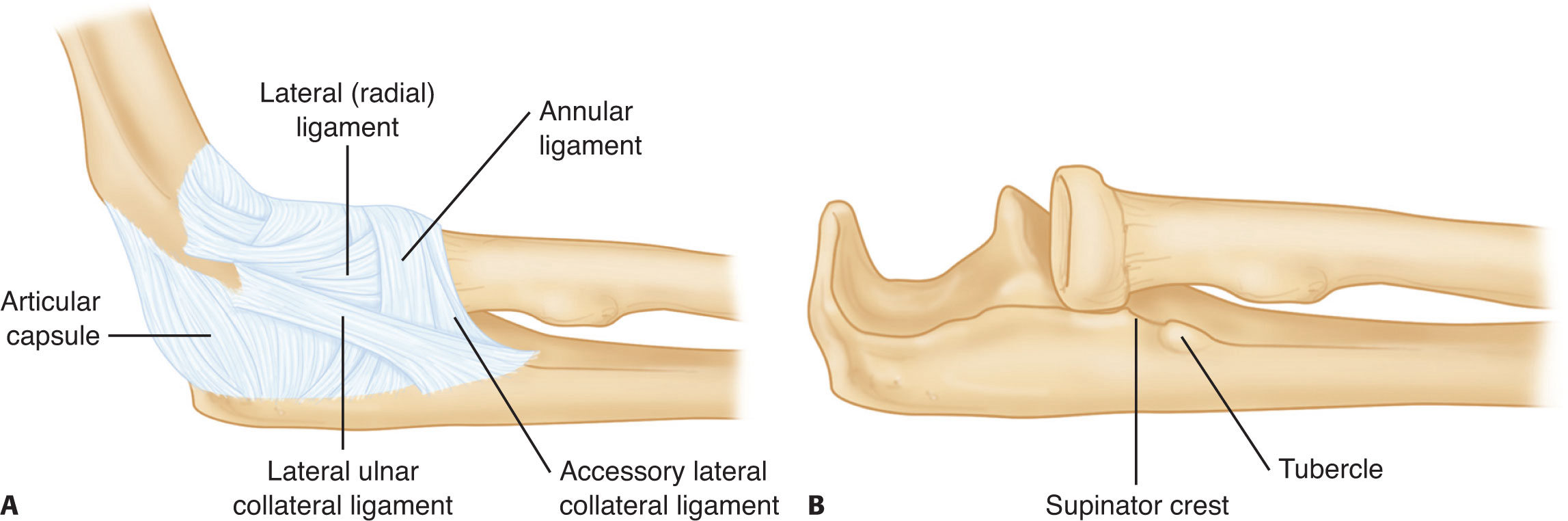
- The LCL complex is made up of four major components: the LUCL, also called the radial ulnohumeral ligament; the RCL proper; the annular ligament; and the accessory collateral ligament. B. Osseous anatomy of the LCL insertion.
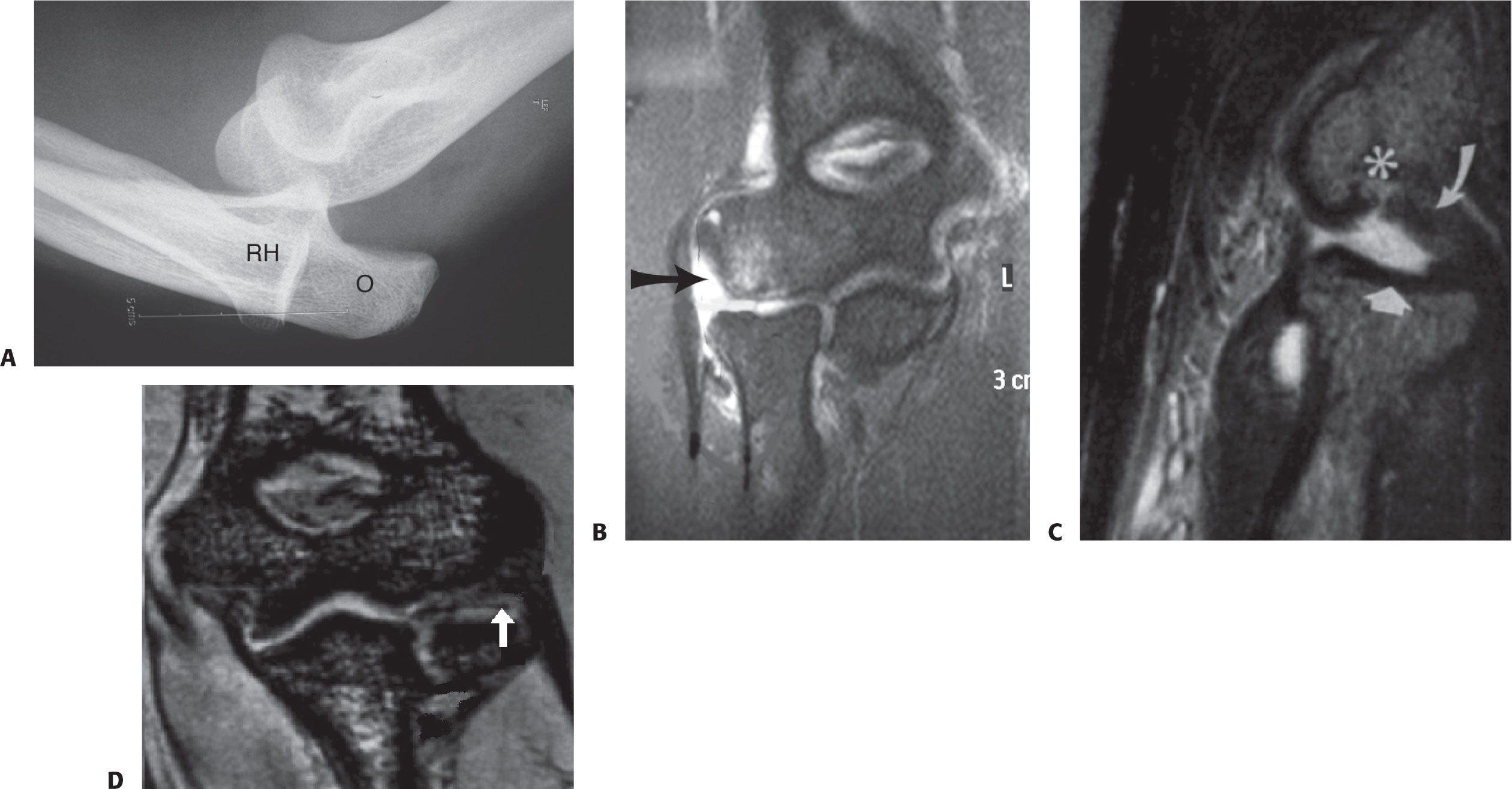
A. Lateral view stress radiograph reveals complete ulnohumeral and radial head (RH) rotatory instability. O, olecranon. B. Coronal oblique view MRI of elbow (with contrast enhancement). LCL disruption can be seen (arrow). C. Sagittal MRI showing Osborne-Cotterill lesion (asterisk and white arrows). D. Coronal MRI showing Osborne-Cotterill lesion (white arrow).