Activity Modification for Arm Injuries
How to keep moving without making things worse — a surgeon's guide to managing the load on an injured shoulder, elbow, wrist or hand.
Activity Modification for Arm Injuries
How to keep moving — without making things worse. A surgeon’s guide to managing the load on an injured shoulder, elbow, wrist or hand.
Why Activity Modification Matters
If you have injured a shoulder, elbow, wrist or hand, one of the most important things you can do is change how you use it for a while. Not stop using it. Not push through. Modify it.
Activity modification is the deliberate, temporary change in how you do something so that an injured tissue can recover while you stay active, working and engaged with life. Done well, it shortens recovery, prevents re-injury and keeps you out of the operating theatre. Done badly, by either over-resting or pushing through, it prolongs symptoms and entrenches the problem.
The Biology Behind the Principle
Tendons, muscles, ligaments and bones are not passive structures. They live, breathe, adapt and remodel based on the loads you place on them. This is the foundation of all sensible rehabilitation.
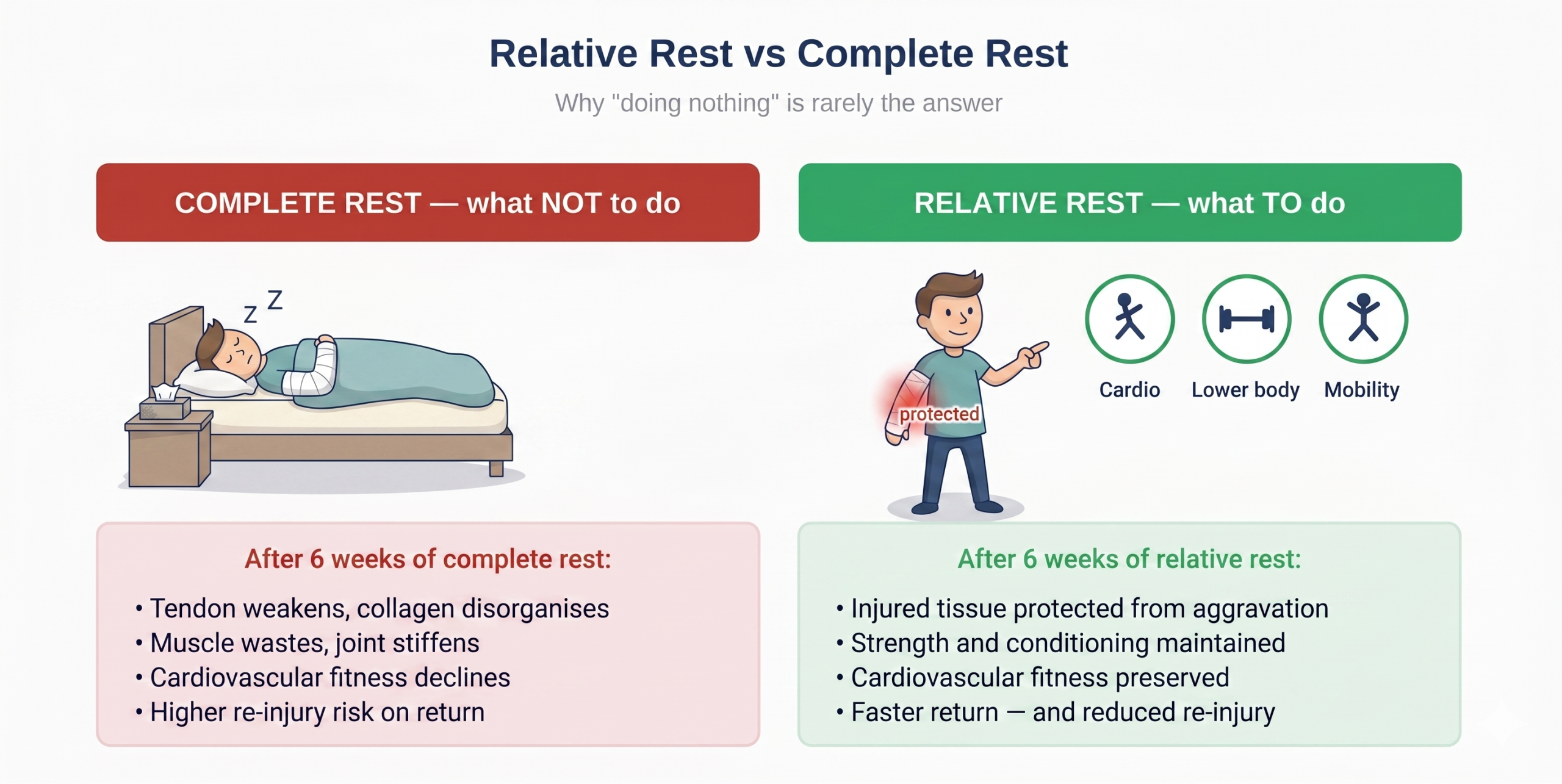
Tissues need load to stay healthy
A tendon completely rested for six weeks loses meaningful strength and stiffness. When you eventually return to activity, the tendon is weaker and more likely to re-injure.
Tissues also need rest from excessive load
Repeated overload with no chance to recover causes microscopic damage to accumulate faster than the body can repair it. Pain persists and can become chronic.
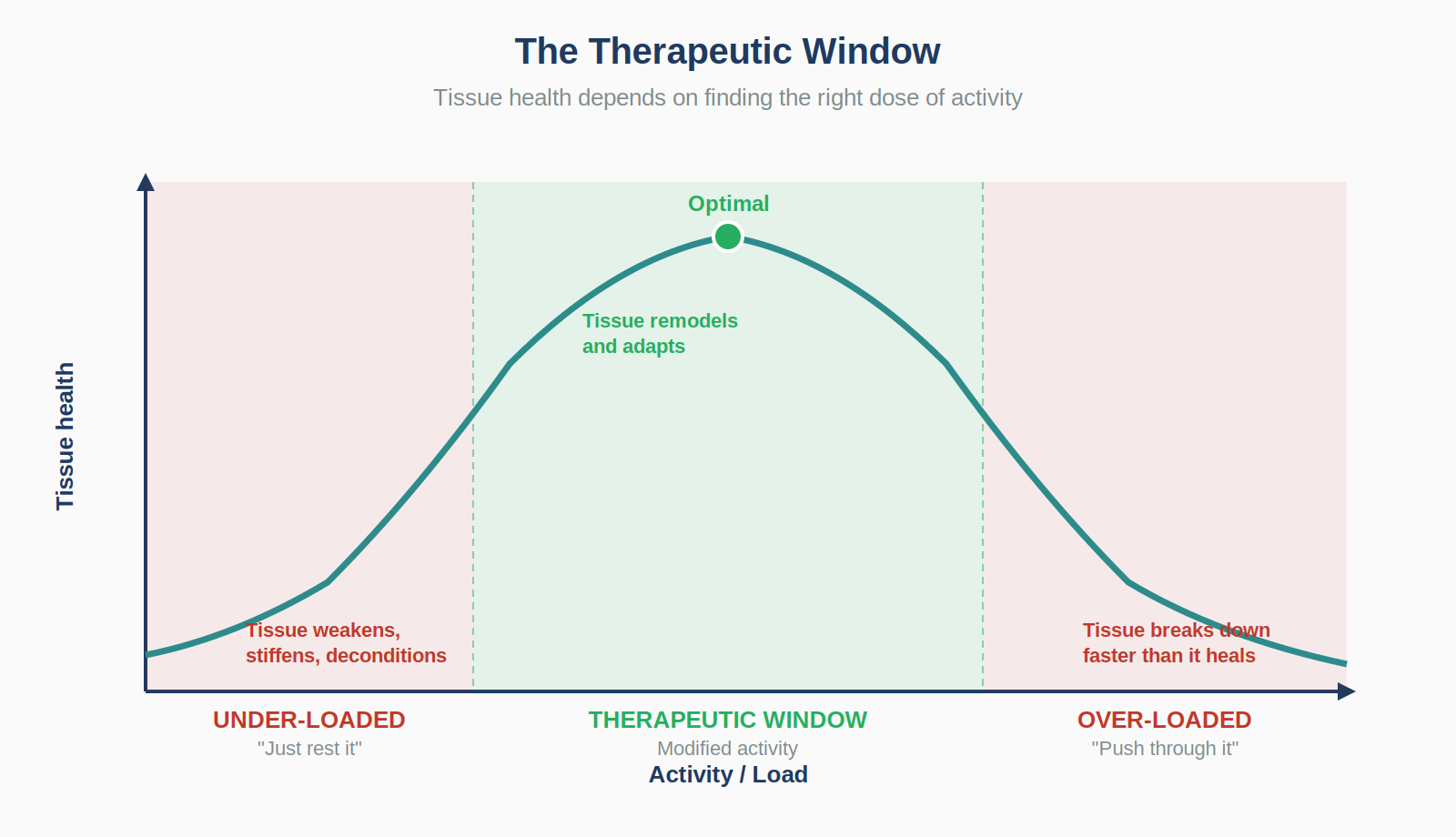
The therapeutic window
Between complete rest and pushing through is the therapeutic window: enough load to maintain and stimulate healing, not so much that you re-injure. Activity modification is the practice of finding and staying in that window.
The Three Principles of Smart Modification
1. Identify the aggravating activity
Spend a week paying close attention. Which movements reproduce pain? What tasks leave you aching that evening or the next morning? Which positions wake you at night? A short symptom diary usually reveals the pattern.
2. Reduce the dose, not the activity
Reduce volume, intensity, frequency or duration to a level the injured tissue can handle. Keep the pattern of movement, but shrink it.
3. Substitute, don’t eliminate
When something cannot be modified to a tolerable level, substitute it. The goal is to keep the body conditioned and the joint moving while one specific motion is rested.
| If this aggravates | Substitute with | Why it works |
|---|---|---|
| Bench press | Floor press, push-up variations | Limits shoulder extension at the painful range. |
| Heavy biceps curls | Hammer curls, rope curls | Reduces strain on the distal biceps tendon. |
| Running with arm swing | Cycling or rowing on a machine | Maintains cardiovascular fitness without arm impact. |
| Gripping work tools | Padded grips, ergonomic handles | Reduces compressive load on tendons. |
| Carrying heavy bags | Backpack with both straps | Distributes load symmetrically. |
| Overhead reaching | Step-stool, repositioned shelving | Avoids the painful arc. |
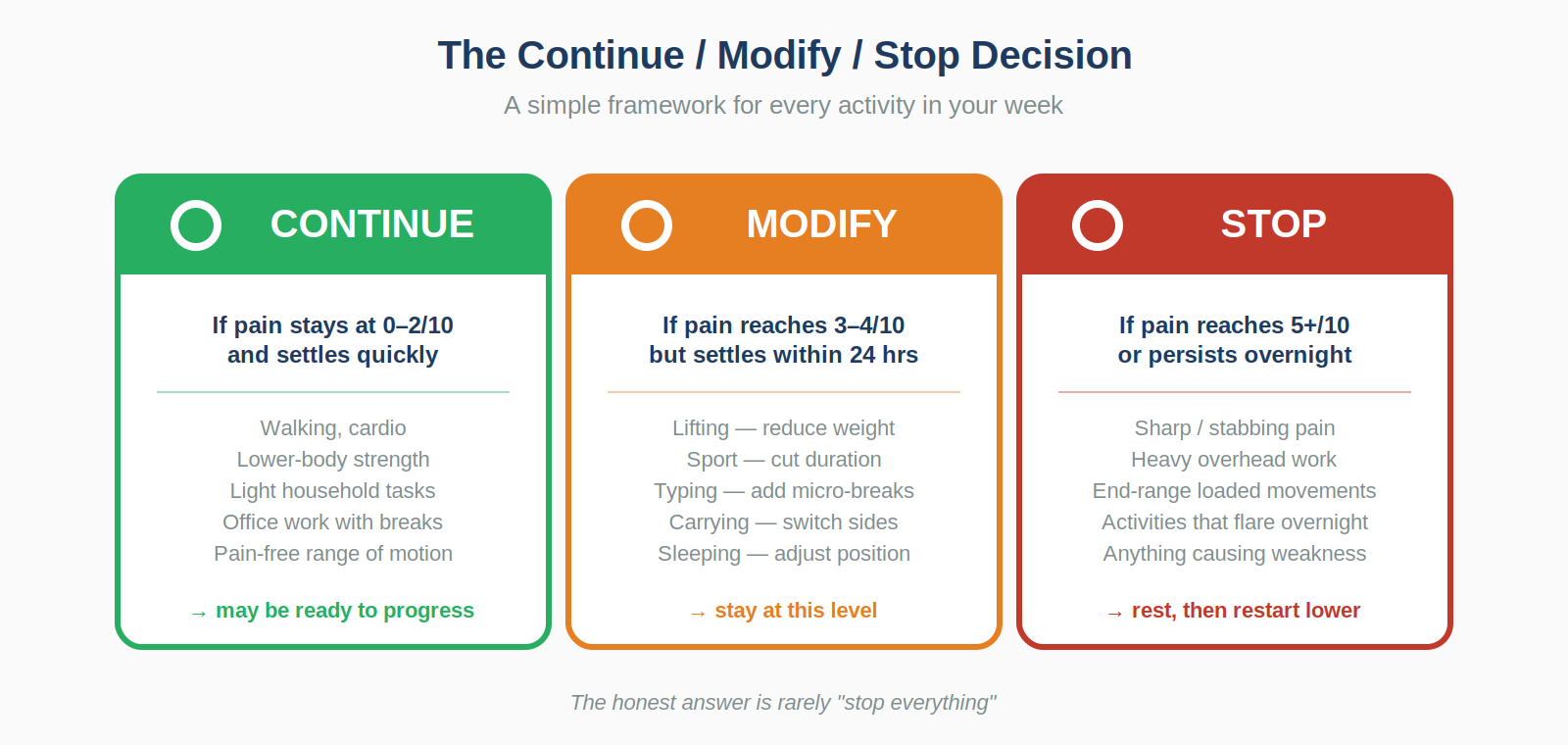
Continue, Modify or Stop?
The simplest decision framework is to place each weekly activity into one of three categories. The honest answer is rarely “stop everything”.
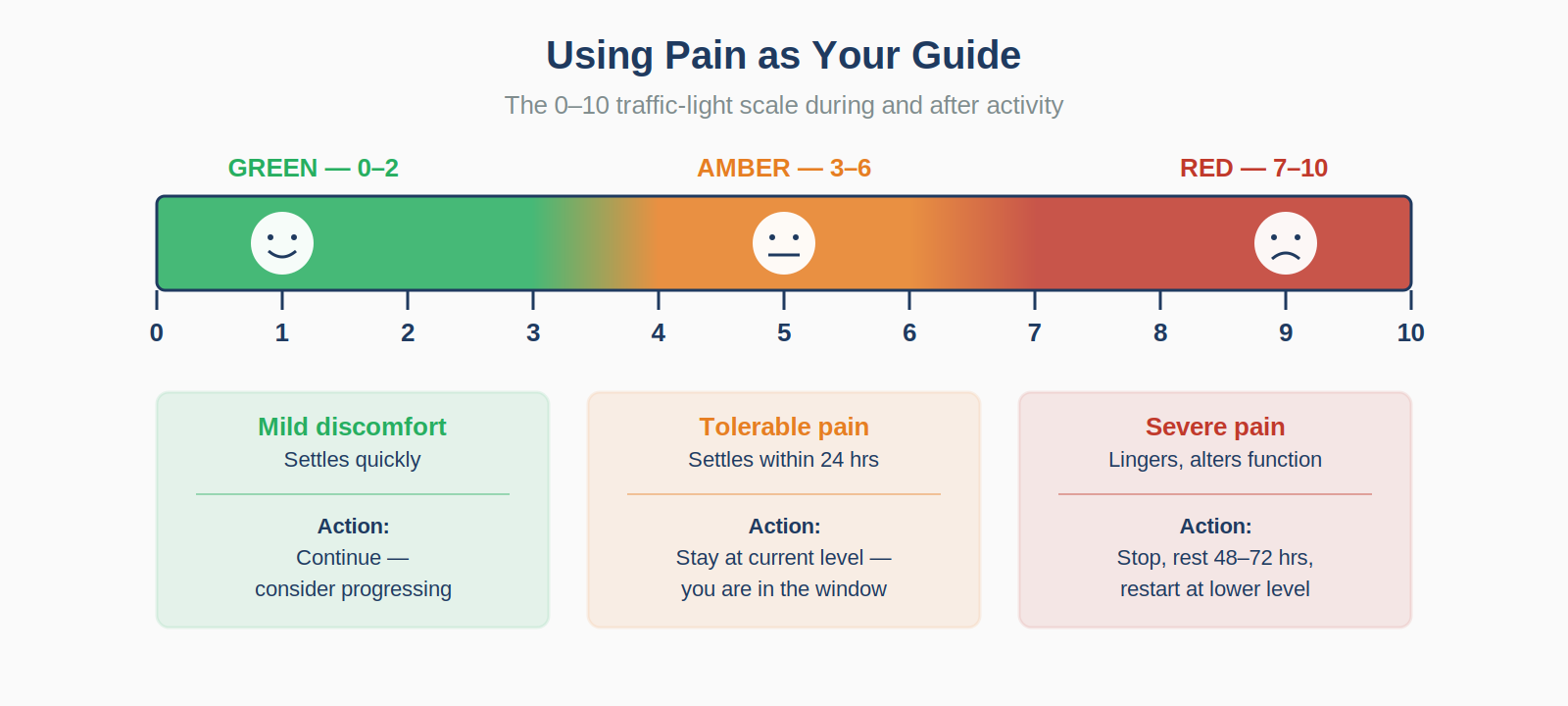
Using Pain as Your Guide
Pain is information. Used well, it tells you when you have moved out of the therapeutic window. Rate your pain during and after activity on a 0-10 scale.
Pain to respect
- Sharp, stabbing, electric or shooting pain.
- Pain at rest or at night, especially if waking you.
- Pain with swelling, redness or warmth.
- Pain that worsens session-on-session.
- Sudden weakness, loss of function, pins, needles or numbness.
Pain to work through — within reason
- Dull ache up to 4/10 during loaded exercise.
- Discomfort that eases as the tissue warms up.
- Stiffness that improves with gentle movement.
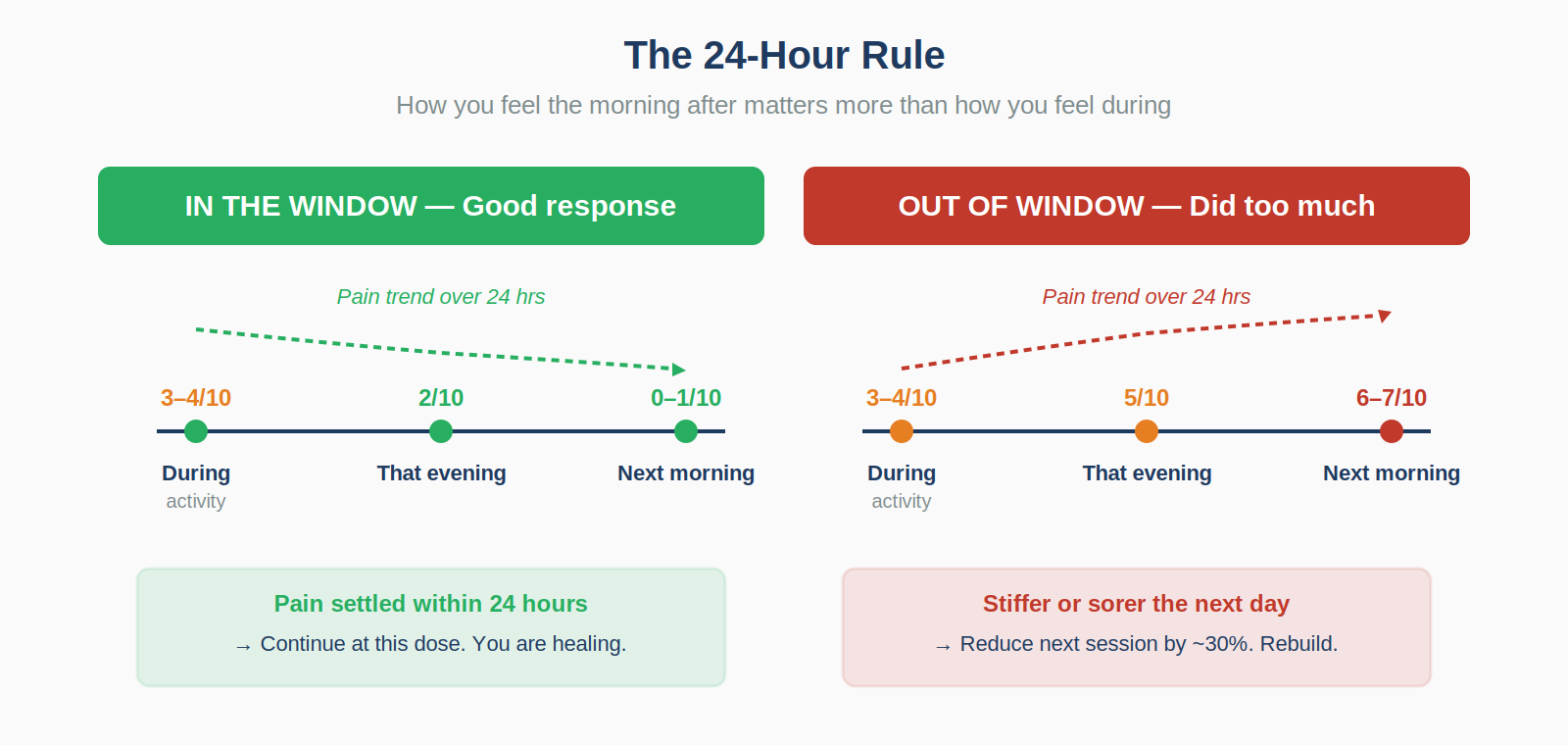
- Mild residual ache that settles within 24 hours.
- Familiar discomfort that improves week-on-week.
Condition-Specific Modifications
Different injuries need different modifications. These are practical changes that often make the biggest difference.
Rotator cuff tendinopathy and shoulder impingement
- Avoid sustained overhead work; break it into 5-minute blocks.
- Keep elbows below shoulder height during weight training.
- Sleep on the unaffected side, hugging a pillow with the painful arm.
- Use “9 and 3” steering wheel position, not “10 and 2”.
- Replace upright rows with face pulls and avoid behind-the-neck exercises.
Frozen shoulder
- Maintain pain-free range with small, frequent movements.
- Avoid sudden grabs or reaching behind the body.
- Dress by sliding the affected arm in first and out last.
- Use heat before, ice after and gentle daily mobility.
- Do not force stretching pain.
Tennis elbow
- Reduce gripping intensity with ergonomic handles and padded grips.
- Lift with the palm facing up rather than down.
- Use a counterforce brace during work or sport.
- Check tennis grip size and string tension.
- Consider a vertical mouse and split keyboard if work-related.
Golfer’s elbow
- Avoid sustained heavy gripping and repetitive wrist flexion.
- Address golf grip pressure and technique with a coach.
- Use neutral-grip or supinated pulls instead of pronated pulls.
- Temporarily substitute heavy deadlifts with lighter trap-bar variations.
Carpal tunnel syndrome
- Wear a neutral wrist splint at night.
- Float the hands while typing; never rest wrists on the desk edge.
- Use a vertical or contoured mouse.
- Take micro-breaks every 20-30 minutes.
- Avoid prolonged vibration or pressure without padded gloves.
De Quervain’s tenosynovitis
- Lift babies with both hands under the trunk, not extended thumbs.
- Use a thumb spica splint during aggravating activities.
- Alternate thumbs and use voice dictation on phones.
- Replace pinch grip with whole-hand grip.
- Wring cloths with two hands rather than twisting one-handed.
Trigger finger / thumb
- Avoid prolonged forceful gripping.
- Use padded gloves or grip sleeves on tools.
- Consider a night splint to keep the digit straight.
- Reduce palm-compressing activities such as long cycling or heavy secateur use.
Thumb base arthritis
- Replace pinch grip with whole-hand power grip.
- Use jar openers, electric tin openers and lever-style handles.
- Avoid wringing wet cloths or twisting tight lids by hand.
- Use a thumb spica brace for flares and prolonged tasks.
Post-fracture or post-surgical recovery
Modification after a fracture or operation must follow the protocol from your surgical team: protected motion, active motion, strengthening, then return to full activity. Do not skip phases or invent new exercises.
Progressing Back to Full Activity
Activity modification is temporary. The goal is to return to what you love doing with tissue that has remodelled and adapted, not tissue that is still vulnerable.
Watch for relapse signals
- Pain returns at the same level after each session.
- Morning stiffness lasts longer than 15-20 minutes.
- Sleep is disturbed by the affected limb.
- New compensatory pain appears in the neck, opposite shoulder or lower back.
- Progress plateaus for more than two weeks.
Returning to sport
- Pain-free in daily life.
- Full or near-full range of motion.
- Strength restored to at least 90% of the unaffected side.
- Training-specific drills tolerated.
- Mental readiness and confidence in the limb.
Common Mistakes I See in Clinic
Doing nothing for weeks, then everything in a day
Complete rest weakens tissue. Reintroduce load early and gradually.
Over-relying on splints and braces
Splints protect when used during aggravating activities or at night. Worn constantly for months, they can cause stiffness and weakness.
Assuming pain medication means it is fixed
Medication can mask pain that would otherwise tell you to slow down. The tissue may still be healing.
Asking the wrong question
Instead of asking “When can I get back to normal?”, ask “What can I do today that gets me closer to normal without setting me back?”
Ignoring the rest of the body
An injured shoulder does not mean an injured cardiovascular system. Keep unaffected limbs strong, legs moving and aerobic fitness up.
When Activity Modification Alone Is Not Enough
Most upper-limb injuries respond well to modification, ergonomic correction, loaded rehabilitation and time. Seek specialist review if any of the following apply.
- Symptoms persist beyond 6-8 weeks despite consistent modification.
- Night pain consistently disrupts sleep.
- Persistent or worsening weakness or muscle wasting.
- Numbness or pins-and-needles that do not settle.
- Sudden injury with significant swelling, bruising or deformity.
- Clicking, catching or locking that is not improving.
These features can suggest a structural problem such as a tear, entrapment or unstable joint that may need imaging or intervention.
A Worked Example: From Flare to Full Recovery
A representative case is a desk worker who develops tennis elbow. The four phases below map onto the recovery pathway.
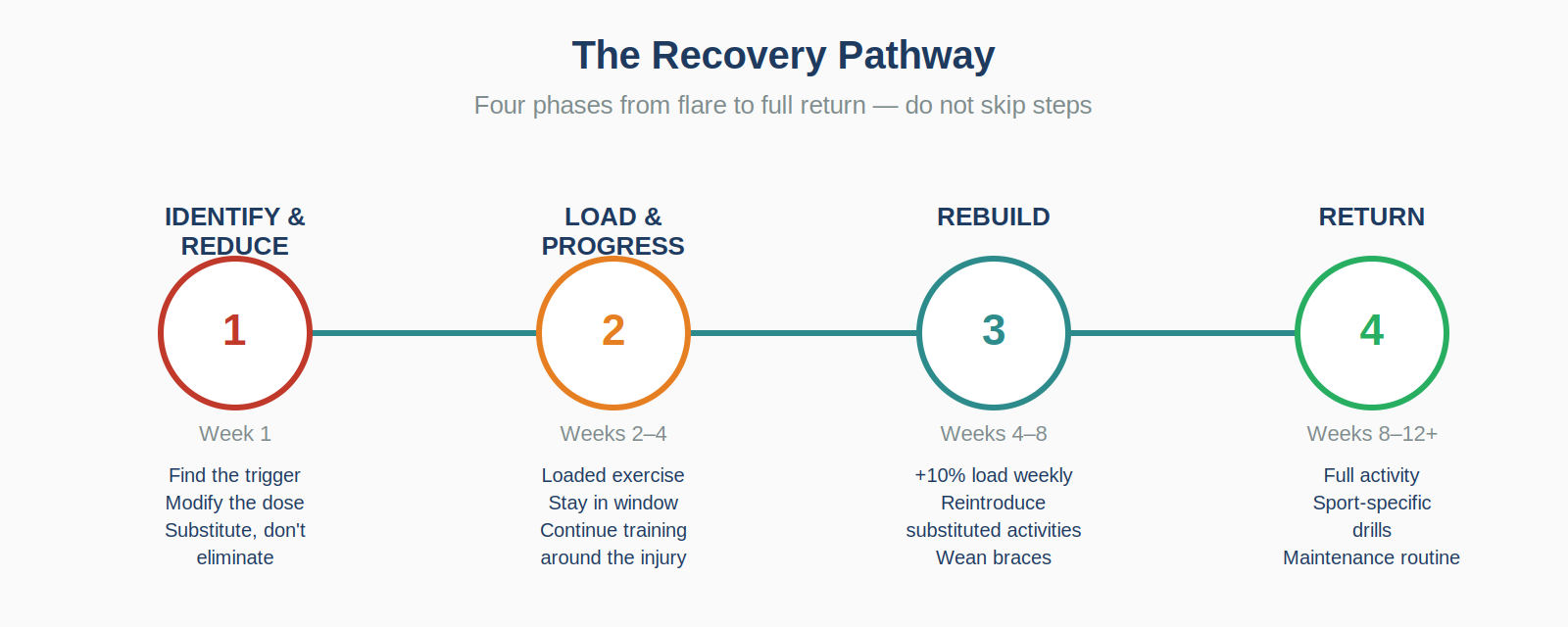
Week 1 — Identify and reduce
- Symptom diary identifies mouse use and heavy gym press as triggers.
- Mouse swapped for a vertical mouse with micro-breaks every 25 minutes.
- Heavy pressing replaced with lower-body strength work and floor presses.
- Counterforce strap used during the working day.
Weeks 2-4 — Load and progress
- Loaded eccentric exercises begin three times weekly.
- Pain during exercise stays around 3/10.
- Mouse work tolerable up to 30 minutes before breaks.
- Cardio and lower-body training continue.
Weeks 4-8 — Rebuild
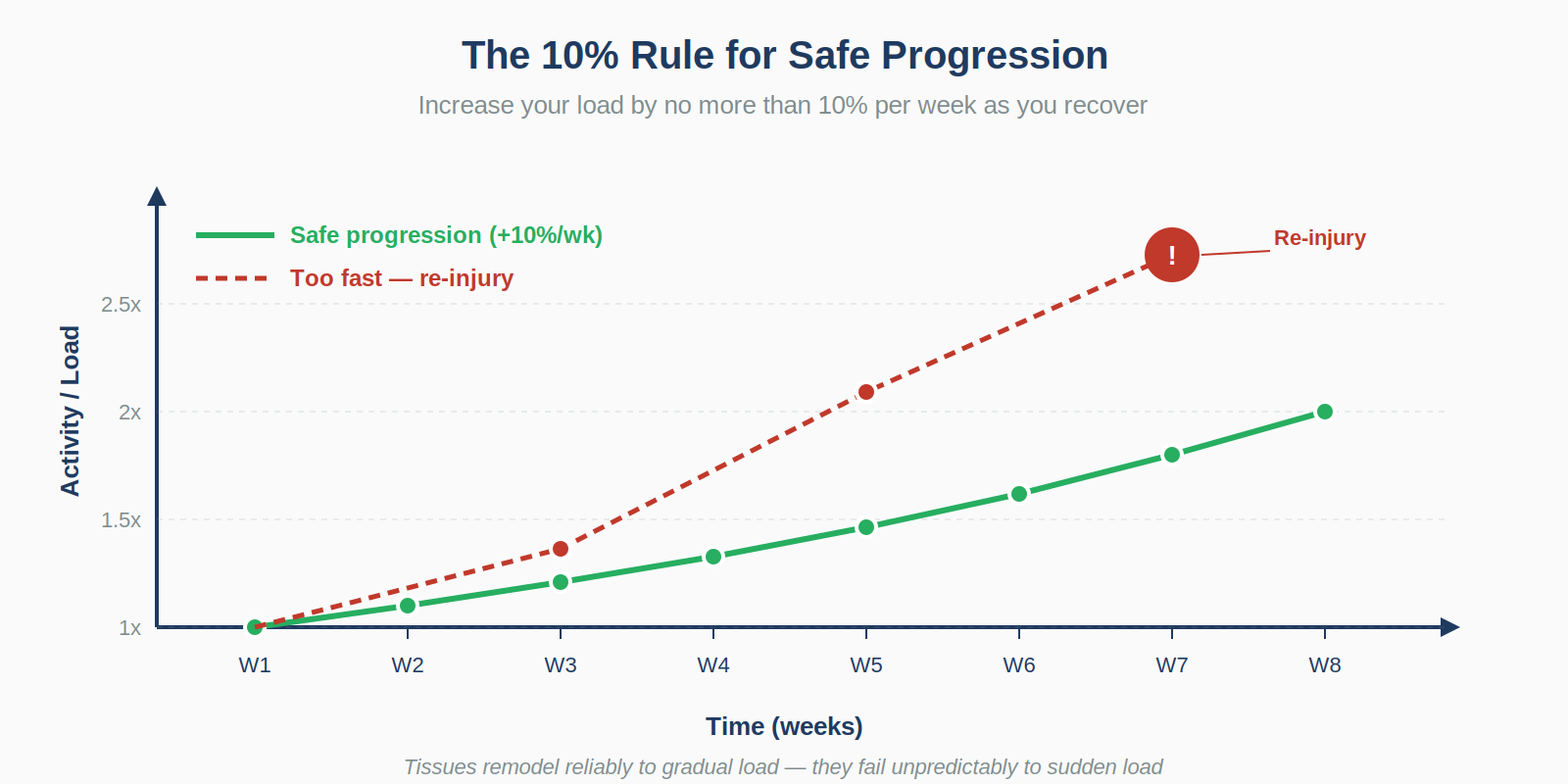
- Exercises increase by around 10% weekly.
- Light upper-body pressing returns with neutral grip.
- Counterforce strap is gradually weaned.
- Daily symptoms become intermittent and mild.
Weeks 8-12 — Return
- Full gym programme returns with attention to grip and elbow position.
- Tennis is reintroduced with coaching on grip and mechanics.
- Symptoms resolve at rest and during normal work.
- Maintenance routine continues.
Frequently Asked Questions
Should I rest completely if it really hurts?
Brief complete rest for 2-3 days may be appropriate for an acute flare. Beyond that, complete rest is rarely the answer. The goal is to find what you can do.
How do I know if I am modifying enough?
If your pain is no worse the next morning, your modification is probably appropriate. If symptoms flare overnight or progress week-on-week, reduce the load.
Can I keep going to the gym?
Almost always, but not necessarily doing the same exercises. Lower-body work, cardio, core and pain-free upper-body movements should usually continue.
What about painkillers and anti-inflammatories?
They can help break a pain cycle, but they are an adjunct, not a treatment. Check with a pharmacist or GP if you have other health conditions or take regular medication.
Should I see a physiotherapist or self-manage?
For a mild recent flare, self-management can work. For persistent symptoms beyond 4-6 weeks, recurrent flares or post-surgical recovery, physiotherapy is valuable.
When will I feel completely normal?
Many upper-limb tendinopathies and overuse injuries take 8-12 weeks of consistent management. Some take longer. Patience is protective.
Is it normal to feel some pain forever?
Most patients return to pain-free function. Some chronic tendon or arthritis problems settle to a lower level of intermittent symptoms, which can still be a successful outcome.
A Final Word
Activity modification is one of the most powerful tools in upper-limb medicine. For most arm injuries, intelligently applied modification, combined with loaded rehabilitation, ergonomic correction and patience, gives the tissue what it needs to heal.
Professor Mohamed A. Imam
Consultant Orthopaedic Surgeon — Upper Limb, Sports Injuries & Complex Trauma
MD, MSc(Hons), PhD, FRCS (Tr & Orth)
This patient information page is provided for educational purposes and does not replace individual medical advice. If you have specific concerns or persistent symptoms, please seek assessment from a qualified healthcare professional.