Spondylolysis (pronounced spon-dee-low-lye-sis) and spondylolisthesis (pronounced spon-dee-low-lis-thee-sis) are prevalent sources of lower back pain among children and adolescents.
Spondylolysis occurs when a vertebra — one of the small bones that form the spinal column — develops a weakness or stress fracture. This condition can affect up to 5% of children as young as six, even without any apparent injury. Adolescents involved in sports that put repeated strain on the lower back, such as gymnastics, football, or weightlifting, are at higher risk of developing this type of stress fracture. In certain instances, the fracture significantly weakens the bone, compromising its stability in the spine. When this happens, the affected vertebra may begin to shift or slip from its position, a condition known as spondylolisthesis.
Anatomy of the Spine
The spine consists of 24 small, rectangular vertebrae stacked sequentially to form a protective canal for the spinal cord. The five vertebrae in the lower back make up what is known as the lumbar spine.
Key components of the spine include:
- Spinal Cord and Nerves: These essential “electrical cables” run through the spinal canal, transmitting signals between the brain and muscles. Nerve roots branch from the spinal cord through openings in each vertebra.
- Facet Joints: Located between and behind neighboring vertebrae, these small joints provide spinal stability and help regulate movement. They function like hinges, aligned in pairs along each side of the spine.
- Intervertebral Disks: Flat, round, and about half an inch thick, these flexible disks sit between vertebrae, acting as cushions and absorbing shock from activities like walking or running.
Understanding Spondylolysis and Spondylolisthesis
Spondylolysis and spondylolisthesis are distinct spinal conditions often closely related.
Spondylolysis Spondylolysis refers to a crack or stress fracture in the pars interarticularis, a narrow section of the vertebra connecting the upper and lower facet joints. This fracture most frequently affects the fifth vertebra in the lumbar spine, though it can also occur in the fourth. The fracture may be unilateral or bilateral.
The pars interarticularis is the vertebra’s most vulnerable area, particularly susceptible to repetitive stress and overuse, common in high-impact sports. Although spondylolysis often affects young athletes, it can develop in people of all ages without any sports-related activity.
Many patients with spondylolysis also experience some degree of spondylolisthesis.
Spondylolisthesis In spondylolisthesis, the fractured pars interarticularis separates, allowing the affected vertebra to slip forward over the vertebra directly below it. This slippage often occurs during periods of rapid growth, such as an adolescent growth spurt.
Doctors classify spondylolisthesis as either low-grade or high-grade based on the extent of slippage. High-grade spondylolisthesis, where more than 50% of the fractured vertebra shifts forward, often results in greater pain and nerve-related symptoms, potentially necessitating surgery to alleviate discomfort and prevent further progression.
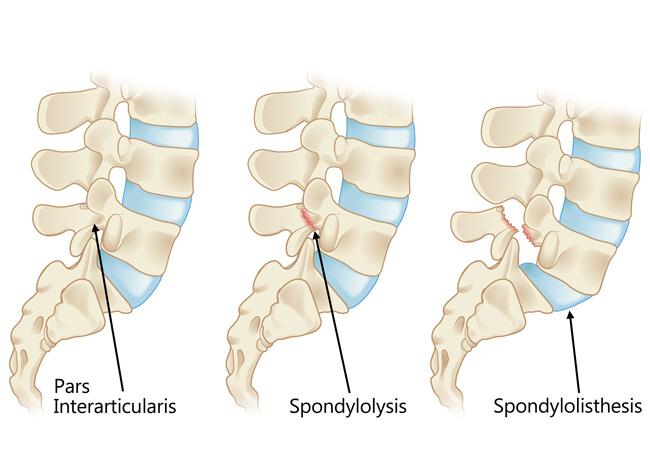
(Left) The pars interarticularis is a narrow bridge of bone found in the back portion of the vertebra. (Center) Spondylolysis occurs when there is a fracture of the pars interarticularis. (Right) Spondylolisthesis occurs when the vertebra shifts forward due to instability from the pars fracture.
Causes of Spondylolysis and Spondylolisthesis
Overuse Both spondylolysis and spondylolisthesis are more prevalent among young athletes involved in sports that require frequent hyperextension of the lower spine, such as gymnastics, football, and weightlifting. Over time, repetitive strain can weaken the pars interarticularis, leading to stress fractures or even vertebral slippage.
Genetics Everyone, regardless of age, faces some level of stress on the lower lumbar spine due to the natural demands of upright walking. However, some individuals may be genetically predisposed to these conditions, as thinner-than-average vertebral bones may increase susceptibility to fractures.
Symptoms of Spondylolysis and Spondylolisthesis
Many individuals with spondylolysis or spondylolisthesis may not exhibit noticeable symptoms, and the conditions are often discovered incidentally through X-rays for unrelated injuries or issues.
When symptoms are present, lower back pain is the most common, often described as:
- Similar to a muscle strain
- Radiating to the buttocks and the back of the thighs
- Aggravated by physical activity and relieved with rest
For those with spondylolisthesis, muscle spasms may cause additional symptoms, including:
- Back stiffness
- Tight hamstrings (muscles along the back of the thigh)
- Difficulty standing or walking
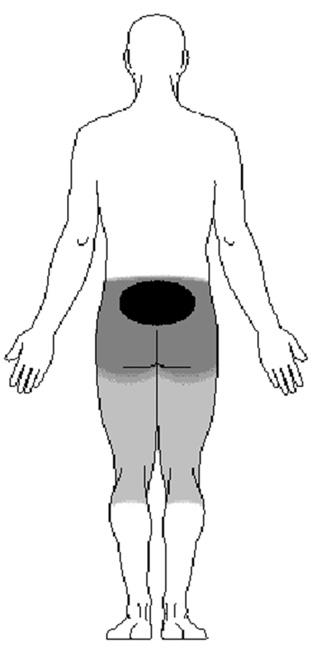
Pain from spondylolysis and spondylolisthesis starts in the center of the lower back and radiates downward.
Doctor’s Examination for Spondylolysis and Spondylolisthesis
Physical Examination During the initial examination, the doctor will take a detailed medical history, asking about the child’s general health, symptoms, and any sports participation, as sports involving intense lower back stress can increase the likelihood of spondylolysis or spondylolisthesis.
The doctor will conduct a thorough examination of the child’s spine and back, assessing for:
- Areas of tenderness
- Range of motion limitations
- Muscle spasms
- Muscle weakness
They will also observe the child’s posture and gait. In some instances, tight hamstrings may cause the child to stand with an unusual posture or walk with a stiff-legged gait.
Imaging Tests for Diagnosing Spondylolysis and Spondylolisthesis
Imaging tests play a crucial role in diagnosing conditions like spondylolysis and spondylolisthesis.
- X-rays: X-rays capture images of dense structures like bones, allowing doctors to examine the spine’s structure. For children suspected of having spondylolysis or spondylolisthesis, multiple X-ray angles may be taken of the lower back to detect stress fractures and assess vertebral alignment. If X-rays reveal a fracture in the pars interarticularis of the fourth or fifth lumbar vertebra, it typically suggests spondylolysis. However, if the gap at the pars has widened and the vertebra has shifted forward, this is indicative of spondylolisthesis. Side-view X-rays are especially useful in assessing the extent of forward vertebral slippage.

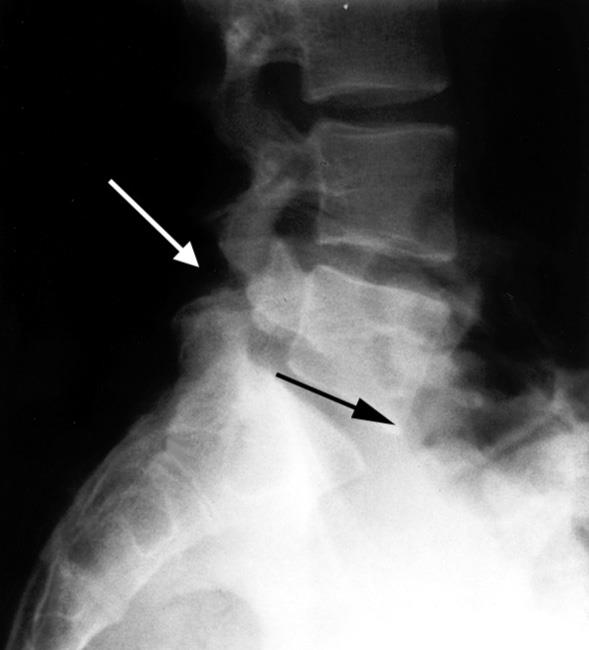
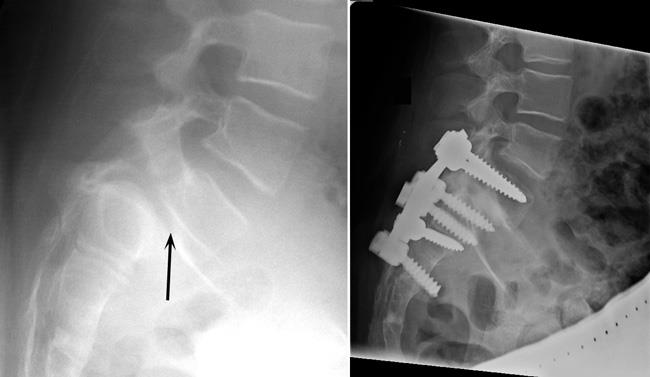
X-ray taken from the side shows a pars fracture in the fifth lumbar vertebra.
Computed Tomography (CT) Scans: CT scans combine X-ray and computer technology to create highly detailed images, providing more information on fractures or vertebral slippage. CT scans are particularly useful for planning treatment, but due to the higher radiation exposure compared to standard X-rays, doctors may not order them routinely. Sometimes, a spondylolysis is incidentally discovered on a CT scan taken for unrelated reasons, such as assessing abdominal pain or post-accident injuries.
- Single Photon Emission Computed Tomography (SPECT) Scans: SPECT scans use a small amount of radioactive material to detect areas of increased bone activity. In cases where CT is unavailable, a SPECT scan can help identify spondylolysis, though this test is now rarely used.
- Magnetic Resonance Imaging (MRI) Scans: MRI scans provide detailed images of soft tissues, unlike X-rays. MRIs are valuable in assessing early degeneration of intervertebral disks or nerve root compression from vertebral slippage. They are also helpful in identifying early-stage pars interarticularis injuries that may not yet be visible on X-rays.
This revision retains the scientific content while optimizing for SEO with terms like “diagnosing spondylolysis,” “vertebral alignment,” “spinal conditions,” and “MRI for back pain,” catering to readers searching for imaging and diagnostic details.
Treatment Options for Spondylolysis and Spondylolisthesis
Treatment for spondylolysis and spondylolisthesis aims to:
- Alleviate pain
- Enable healing of recent pars fractures
- Support a safe return to sports and regular activities
Nonsurgical Treatments
Most patients with spondylolysis and mild spondylolisthesis experience improvement with nonsurgical treatments, which may include:
- Rest: Avoiding high-impact sports and activities that strain the lower back helps reduce symptoms and allows time for recovery.
- Nonsteroidal Anti-Inflammatory Drugs (NSAIDs): Medications like ibuprofen and naproxen can minimize swelling and relieve pain.
- Physical Therapy: A tailored program including flexibility exercises, hamstring stretches, and core strengthening can enhance mobility and support the spine.
- Bracing: Some patients may benefit from wearing a back brace to restrict spinal movement and promote healing of recent pars fractures. Bracing is typically effective for those with a sudden onset of pain; however, it is less helpful for long-standing pain, where the fracture is less likely to heal even with prolonged brace use.
Throughout treatment, periodic X-rays may be taken to monitor vertebral alignment and check for any changes in position.
Surgical Treatment
Surgery may be recommended for spondylolisthesis patients who have:
- Significant vertebral slippage
- Progressive worsening of the condition
- Persistent back pain unresponsive to nonsurgical treatment
Spinal Fusion Surgery
Spinal fusion, the most common surgical approach for spondylolisthesis, involves permanently connecting the affected vertebrae to stabilize the spine and reduce pain. The main objectives are to:
- Halt further vertebral slippage
- Stabilize the spine
- Relieve severe back pain
Surgical Procedure
Spinal fusion works by fusing the affected vertebrae into a single, solid bone, eliminating movement in the painful spinal segment. To perform the fusion, the surgeon first realigns the vertebrae, then places small bone grafts between them to encourage natural bone growth over time, similar to how a fracture heals.
For added stability, metal screws and rods may be used to secure the vertebrae during healing. In cases of severe slippage with nerve root compression, the surgeon may expand the spinal canal to relieve nerve pressure before proceeding with the fusion.
Expected Outcomes for Spondylolysis and Spondylolisthesis
Most patients with spondylolysis or spondylolisthesis achieve significant relief from pain and symptoms, often within weeks or a few months. In the majority of cases, they can gradually return to sports and daily activities with minimal risk of complications or recurrence.
To reduce the likelihood of future injuries, doctors often recommend specific exercises to improve flexibility and strengthen core and back muscles. Routine check-ups are also essential to monitor spinal health and ensure long-term stability and well-being.