Lumbar spinal canal narrowing is a frequent source of lower back pain and leg discomfort, often leading to sciatica symptoms.
As the body ages, natural wear-and-tear can gradually reduce the width of the spinal canal, which encases the spinal nerves and spinal cord—a condition known as spinal stenosis. Degenerative spinal changes are common, appearing in as many as 95% of individuals by age 50, and lumbar spinal stenosis predominantly affects adults over 60. Both men and women experience similar rates of nerve root compression.
In rare cases, some individuals are born with spinal structures that predispose them to lumbar spinal stenosis, referred to as congenital spinal stenosis. This typically occurs in people with a naturally smaller spinal canal, where restricted space makes them more susceptible to early degeneration or arthritis. This form of stenosis is more common in men, with symptoms generally beginning between ages 30 and 50.
Anatomy
The spine consists of a series of small bones, called vertebrae, stacked along the back to form a sturdy column. Alongside these vertebrae, the spine comprises muscles, ligaments, nerves, and intervertebral discs, all essential for stability, flexibility, and protection.
A basic understanding of spine structure and function is key to grasping spinal stenosis. For an overview of spine anatomy, visit our section on Spine Basics.
Description
Spinal stenosis develops when the space surrounding the spinal cord and nerves becomes restricted. This narrowing can place pressure on the spinal cord and nerve roots, often resulting in pain, numbness, or leg weakness.
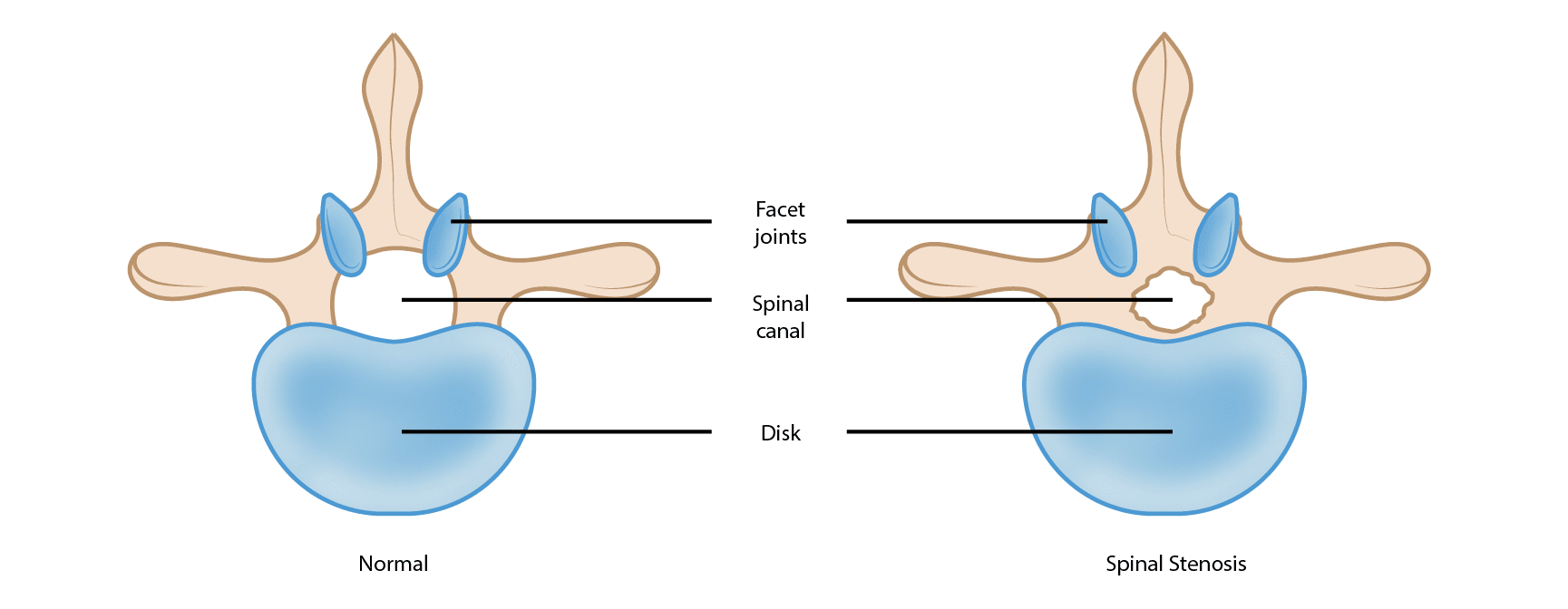
This illustration shows a healthy vertebra (cross-section view) and a vertebra with narrowing of the spinal canal, called stenosis.
Cause
The primary cause of spinal stenosis is arthritis, which involves the degeneration of joints throughout the body.
In the spine, arthritis can develop as intervertebral discs deteriorate and lose moisture. Discs in children and young adults are typically rich in water, maintaining their flexibility and cushioning abilities. However, as we age, these discs gradually dry out and weaken. This degeneration can lead to disc settling or collapse, resulting in reduced disc height and contributing to spinal canal narrowing.
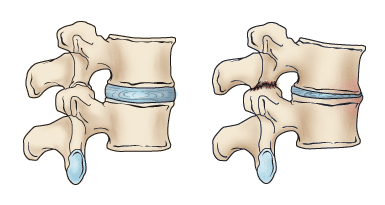
When we are young, disks have a high water content (left). As disks age and dry out, they may lose height or collapse (right). This puts pressure on the facet joints and may result in arthritis
Arthritic bone spurs narrow the spinal canal.
Symptoms
- Back Pain: Individuals with spinal stenosis may experience back pain, though the presence and intensity can vary based on the severity of arthritis in the spine.
- Burning Pain in Buttocks or Legs (Sciatica): Nerve compression in the spine may lead to pain in the areas supplied by these nerves, often described as an aching or burning sensation. Typically, the pain originates in the buttocks and radiates down the leg, and in advanced cases, it can extend to the foot.
- Numbness or Tingling in Buttocks or Legs: Increased nerve pressure may cause numbness and tingling alongside the burning pain, although not everyone will experience both symptoms simultaneously.
- Leg Weakness or Foot Drop: When nerve compression reaches a significant level, weakness may develop in one or both legs. Some people may experience foot drop, where lifting the front of the foot becomes difficult, resulting in the sensation that the foot “slaps” against the ground while walking.
- Acute Cauda Equina Syndrome: This uncommon but serious condition is a medical emergency requiring immediate attention. Severe nerve compression can cause numbness in the groin area, loss of bowel or bladder control, and leg weakness that impedes walking. These symptoms indicate the need for emergency surgery.
In spinal stenosis, leaning forward or sitting often relieves discomfort, as studies suggest that these positions can expand the space available for nerves in the lumbar spine. Pain generally intensifies when standing straight or walking. Some individuals find they can comfortably use a stationary bike or walk with support, like leaning on a shopping cart. However, walking for more than 1 or 2 blocks may provoke severe sciatica or leg weakness.
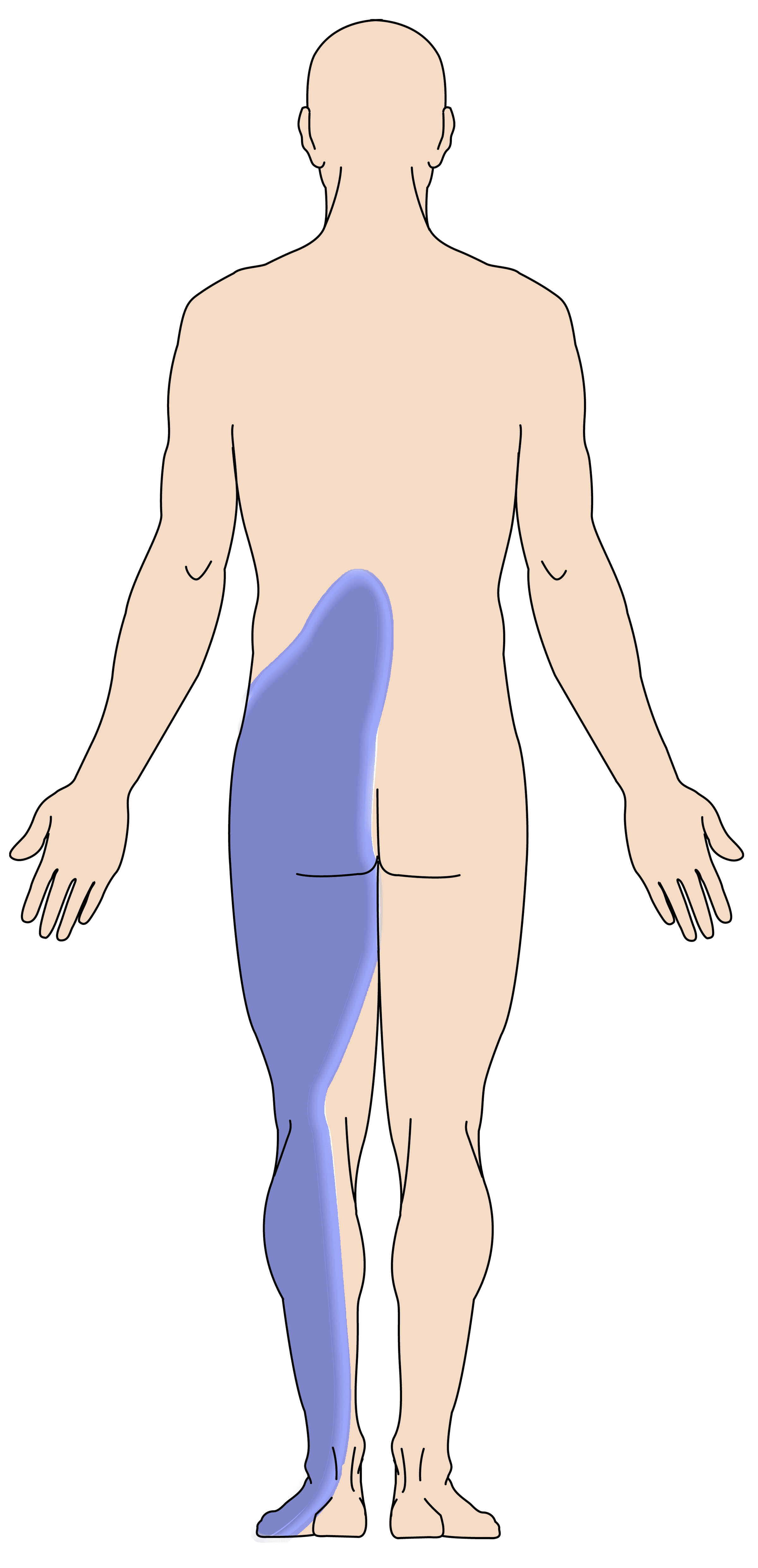
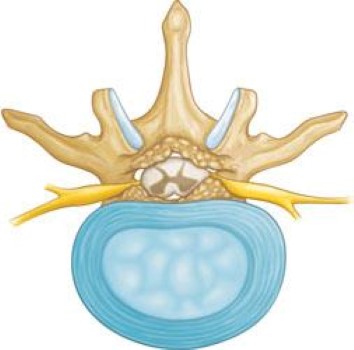
Spinal nerves relay sensation in specific parts of your body. Pressure on the nerves can cause pain in the areas that the nerves supply, including pain in the buttocks that radiates down the leg — called sciatica.