What are Metacarpal Fractures?
Metacarpal fractures refer to breaks in the bones of the hand that form the base of the fingers. These fractures can occur at the base, shaft, neck, or head of the metacarpals, leading to issues like shortening, rotation, or angulation of the bone. Since the metacarpals provide a foundation for finger movement, any injury to these bones can significantly impact the function of the hand.
Understanding Metacarpal Anatomy
Thumb Metacarpal (First Metacarpal)
- Independence: The thumb metacarpal is highly independent and is stabilized by its carpometacarpal (CMC) joint and supporting muscles.
Other Metacarpals (Second to Fifth)
- Connection: These metacarpals are tightly connected through the CMC joints at their base and the deep transverse metacarpal ligaments at their heads.
- Ligaments: The deep transverse metacarpal ligaments play a crucial role in preventing fracture shortening and rotation, especially in the central metacarpals (third and fourth).
Structural Shape
- Thumb Metacarpal: It has a round cross-sectional shape.
- Other Metacarpals: These have a triangular shape with dorsal, anterolateral, and anteromedial facets
Muscle and Tendon Coverage
- Interosseous Muscles: Cover each metacarpal’s radial and ulnar surfaces, providing blood supply but also being at risk of contracture in severe hand injuries.
- Extensor Tendons: Lie just above the base and shaft of each metacarpal and contribute to the dorsal extensor apparatus of each finger
Vascular and Nerve Structures
- Deep Palmar Arch and Ulnar Nerve: Located just volar (toward the palm side) to the metacarpals and are at risk during fractures and surgeries.
Joint Structure
- Collateral Ligaments: Arise from fossae and tubercles on either side of the metacarpal head, contributing to the stability of the metacarpophalangeal (MP) joint.
Causes and Types of Metacarpal Fractures
Common Injury Mechanisms
- Axial Load: Often leads to fractures due to direct force along the bone’s length.
- Torsional Injuries: Result in long oblique fractures with a risk for malrotation.
- Direct Impact: Causes short transverse fractures.
- Crush Injuries: Can lead to a combination of fractures with an increased risk of compartment syndrome and significant stiffness.
Specific Types of Fractures
- Boxer’s Fracture: Fracture of the neck of the fifth metacarpal with a flexed, apex dorsal angulation
- Oblique Fractures: Often due to twisting forces, leading to potential malrotation
- Transverse Fractures: Caused by direct impacts
- Complex Fractures: Seen in crush injuries with multiple fracture patterns and higher risks of complications

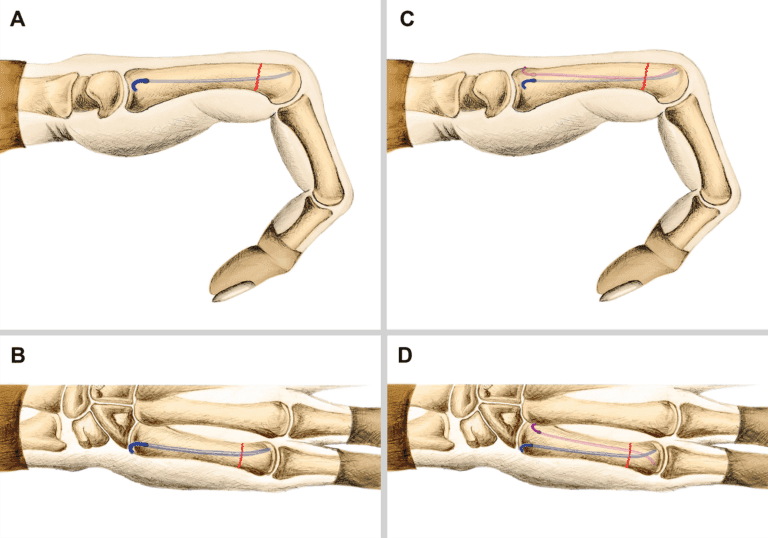
- A. Angled metacarpal shaft fractures deserve an attempt at closed reduction. B. Jahss maneuver. A dorsally directed force is applied to the flexed PIP joint while the metacarpal is stabilized proximally. C. Metacarpal neck reduction applying force at the metacarpal head while stabilising the metacarpal shaft proximally. D. Fourth metacarpal shaft fracture reduction is being stabilised with pressure directly on the metacarpal head. Note the MP joint is maintained in extension. E. MP flexion on the day of cast removal after being cast for 4 weeks.
Treatment Strategies
Nonoperative Treatment
- Indications: Suitable for stable, nondisplaced fractures.
- Methods: Includes immobilisation with a cast or splint, followed by physical therapy to restore function.
Operative Treatment
Open Reduction and Internal Fixation (ORIF)
- Purpose: To align and stabilise the bones using plates, screws, or wires.
- Procedure:
- Incision: Made over the fracture site.
- Reduction: Bones are realigned to their proper position.
- Fixation: Hardware is used to hold the bones in place during healing.
Fragment Excision
- Purpose: Removal of small bone fragments that cannot be fixed.
- Procedure: Performed when fragments are too small or numerous for internal fixation.
Radial Head Excision or Replacement
- Purpose: Used in severe cases where the radial head is irreparably damaged.
- Procedure: Involves removing or replacing the radial head with a prosthesis.
Recovery and Rehabilitation
- Postoperative Care: Includes immobilisation, pain management, and gradual movement introduction.
- Physical Therapy: Essential to regain strength and flexibility in the hand and fingers.
- Follow-Up: Regular check-ups to monitor healing and adjust treatment as necessary.
Conclusion
Metacarpal fractures require careful evaluation and a tailored treatment approach to ensure proper healing and restoration of hand function. Depending on the severity and complexity of the fracture, treatment may range from non-surgical methods to surgical interventions like ORIF. Proper postoperative care and rehabilitation are crucial for achieving the best outcomes. Always follow your doctor’s advice and attend follow-up appointments to ensure optimal recovery.