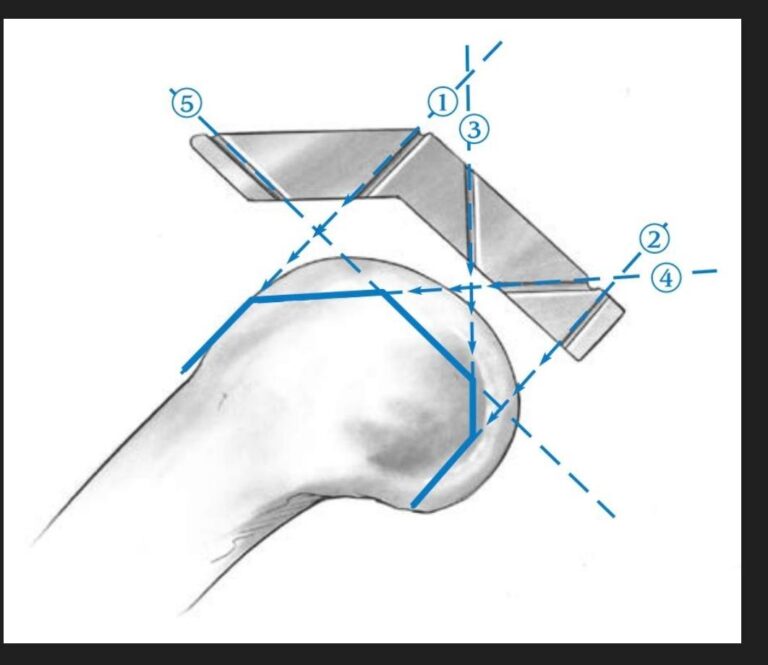
1. Anterior Femoral Cut (Line 1)
- Purpose:
- This cut defines the position of the anterior flange of the femoral component, which is essential for smooth movement of the patellofemoral joint.
- It prevents abnormal pressure or friction between the femoral component and anterior soft tissues.
- Complications of Incorrect Cuts:
- Over-resection: Leads to notching, or erosion of the anterior femoral surface, increasing the risk of fractures in this area.
- Under-resection: Causes patellofemoral overstuffing, leading to anterior knee pain during activities like stair climbing.
- Symptoms of Errors:
- Anterior knee pain during flexion or walking.
- Difficulty ascending or descending stairs due to patellar impingement.
- Error Detection:
- Clinically:
- Assess for anterior knee pain on compression.
- Evaluate range of motion.
- Radiologically:
- Use lateral X-ray to confirm the anterior angle’s integrity and check for notching or excessive patellar pressure.
- Clinically:
2. Posterior Femoral Cut (Line 2)
- Purpose:
- Controls the flexion gap, ensuring knee stability during flexion.
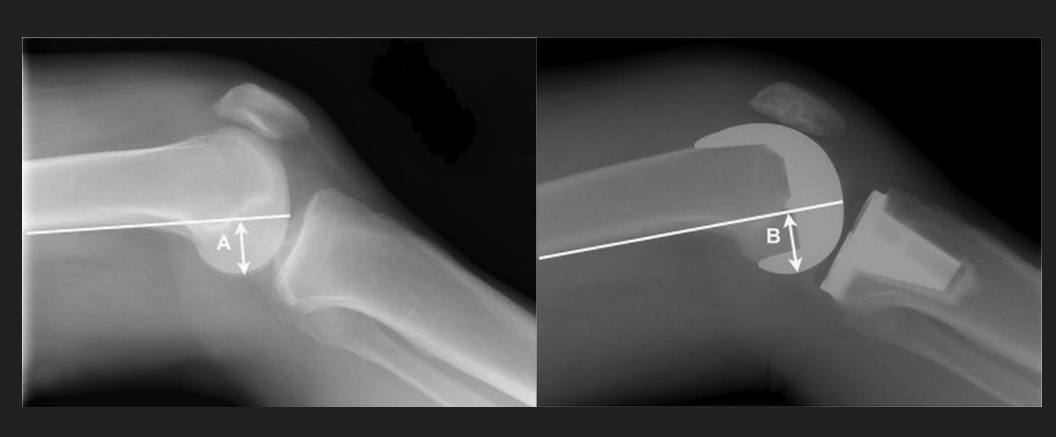
- Maintains the posterior condylar offset for proper knee function.
- Complications of Incorrect Cuts:
- Over-resection: Results in an enlarged flexion gap, causing flexion instability.
- Under-resection: Narrows the flexion gap, restricting knee flexion and leading to stiffness.
- Symptoms of Errors:
- Instability during daily activities like sitting or standing.
- Difficulty achieving full knee flexion accompanied by posterior pain.
- Error Detection:
- Clinically:
- Perform anterior-posterior stability tests at 90° flexion.
- Assess knee movement during stair navigation.
- Radiologically:
- Use lateral X-ray to examine posterior tibial slope and flexion gap balance.
- Clinically:
3. Posterior Chamfer Cut (Line 3)
- Purpose:
- Stabilizes the posterior flange of the femoral component and ensures proper adaptation to the posterior femoral surface.
- Complications of Incorrect Cuts:
- May lead to instability of the posterior component, causing impingement between the component and soft tissues like posterior tendons.
- Symptoms of Errors:
- Posterior knee pain during flexion or extension.
- Limited knee movement due to posterior component impingement on soft tissues.
- Error Detection:
- Clinically:
- Assess posterior knee pain during activities.
- Test range of motion.
- Radiologically:
- Use lateral X-ray to evaluate the alignment and adaptation of the posterior component to the femoral surface.
- Clinically:
4. Anterior Chamfer Cut (Line 4)
- Purpose:
- Facilitates fixation of the anterior chamfer and minimizes excessive pressure on anterior soft tissues.
- Complications of Incorrect Cuts:
- Over-resection: Can interfere with anterior soft tissues, such as the patella or tendons.
- Under-resection: Results in improper adaptation of the femoral component to the anterior surface, causing discomfort.
- Symptoms of Errors:
- Anterior knee pain during daily activities.
- Difficulty flexing the knee with a sensation of obstruction.
- Error Detection:
- Clinically:
- Test anterior knee motion during activities like running or jumping.
- Assess for anterior pain.
- Radiologically:
- Use lateral X-ray to verify the anterior angle and its alignment with the femur.
- Clinically:
5. Distal Femoral Cut (Line 5)
- Purpose:
- Controls mechanical alignment and balances the extension gap.
- Ensures even load distribution between flexion and extension.
- Complications of Incorrect Cuts:
- Over-resection: Causes excessive extension gap, leading to instability during standing.
- Under-resection: Leads to difficulty in full knee extension (flexion contracture), restricting movement.
- Symptoms of Errors:
- Inability to fully extend the leg.
- Feeling of instability while standing or walking.
- Error Detection:
- Clinically:
- Examine full leg extension using alignment tests.
- Evaluate knee pain during standing.
- Radiologically:
- Use AP X-ray to assess mechanical axis alignment and lateral X-ray for component adaptation.
- Clinically:
Postoperative Evaluation
- Clinical Examination:
- Assess range of motion and knee stability.
- Check for localized pain or swelling around the joint.
- Radiological Evaluation:
- AP X-ray: Evaluate mechanical axis and component balance.
- Lateral X-ray: Inspect anterior and posterior alignment.
- Axial X-ray: Assess femoral component alignment with the patella.
Conclusion:
Accurate surgical cuts during total knee arthroplasty are fundamental to achieving joint stability and preventing clinical symptoms. Any errors in planning or execution can result in complications such as instability, restricted motion, or chronic pain, which can be identified through thorough clinical and radiological assessments.