Spinal fusion is among the most frequently performed procedures for stabilizing painful or unstable spinal bones, whether in the neck or back. The primary goal is to join these bones to encourage them to heal as a unified, solid structure. Achieving this fusion requires the use of additional bone material, known as a bone graft.
For bone fusion to occur, several essential conditions must be met:
- Structural Stability: Bone formation requires a stable environment. Screws, rods, and/or plates are often employed to provide the necessary support during fusion.
- Bone Formation Elements: Effective bone grafting needs three critical elements: cells capable of forming bone, proteins to stimulate bone growth, and a scaffold for new bone to attach. If a bone graft possesses all these attributes, it can promote successful bone formation. However, if a graft material lacks one or more of these properties, it may need to be combined with other graft materials for optimal results.
Today, a variety of bone graft options are available. The most suitable graft or graft combination depends on factors such as the specific spinal segment requiring fusion, the patient’s age, and overall health. Your surgeon will review and discuss the best grafting options tailored to your individual needs.
Types of Bone Grafts
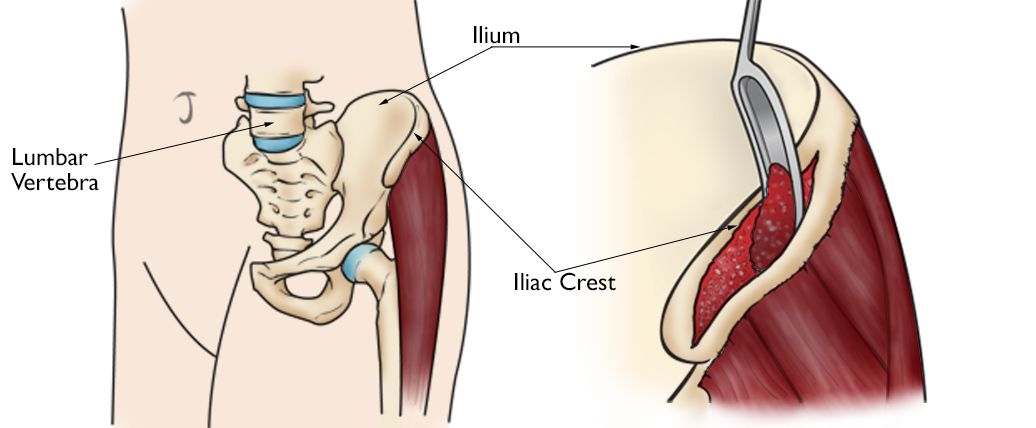
Autograft An autograft is a widely used technique in spinal fusion surgery, involving the transfer of bone from one area of the patient’s body to another, typically to support fusion in the spine. This process, known as harvesting and grafting, often uses bone from a location that won’t be significantly affected by its removal, such as the iliac crest—the edge of the pelvic bone. The surgeon carefully extracts the bone from this area using specialized instruments.
Although the iliac crest autograft has proven effective, it does have certain drawbacks:
- Pain may occur at the harvesting site, sometimes persisting for an extended period post-surgery.
- The iliac crest provides a limited supply of bone, particularly as aging leads to natural bone thinning and weakening.
- There is a risk of fracture or breakage at the iliac crest.
- Potential complications include infection or bleeding.
With advancements in surgical techniques, this method is now less commonly used. However, it remains an option for high-risk patients, such as those with a history of unsuccessful fusion, smokers, or individuals with other factors that may hinder healing.
One significant benefit of the iliac crest autograft is its rich composition of cells, proteins, and scaffolding elements essential for bone healing. Minimally invasive techniques may be employed to reduce trauma at the graft site, potentially lowering the associated pain.
Local Bone Autograft In some spinal fusion surgeries, portions of the spinal bones are removed to alleviate nerve pressure. This removed bone is often preserved and reused as a graft, effectively recycling it from a non-essential area to the intended fusion site.
Advantages of using local bone include:
- It is the patient’s own bone, eliminating the risk of rejection.
- No additional incisions are necessary.
- It avoids hip-related pain associated with iliac crest harvesting.
- Like the iliac crest autograft, it contains the essential components for successful bone fusion.
However, a limitation of this approach is that the spinal bones are relatively small, providing only a limited amount of bone for grafting.
Cadaver or Allograft Bone
Many spinal surgeons opt to use donor or cadaver bone, a type of graft known as an allograft, typically sourced from a bone bank. Like organ donation, bone can be donated upon a person’s death.
Allografts have a long history in spinal fusion procedures. Unlike autografts taken directly from a patient, allografts do not produce new bone; instead, they serve as a scaffold that encourages natural bone to grow over their surface, which eventually replaces the donor bone over time.
Advantages of using allografts include:
- Availability in various shapes and sizes, which allows for precise fitting in the required spinal area.
- Allografts are effective in supporting bone healing in most cases.
- Since the donor bone functions solely as a scaffold, rejection is rare, eliminating the need for growth-stimulating cells or proteins.
- The risk of disease transmission from donor bone is extremely low.
Allograft Stem Cells
Stem cells derived from either donor or cadaver sources provide additional support for bone fusion. As undifferentiated cells capable of forming bone, they offer a minimal risk of tissue rejection due to their basic cellular structure.
Current research shows promising fusion rates with allograft stem cells, though long-term comparisons to other graft types are still pending. Although these materials possess the three essential properties for bone formation, they may not have sufficient living cells to form bone independently, often necessitating a combination with other graft types for optimal results.
Demineralized Bone Matrix (DBM)
DBM is processed bone with its calcium content removed. This process reveals vital proteins that stimulate bone healing.
The downside is that DBM lacks bone-forming cells. Similar to other allografts, DBM functions as a scaffold to support bone growth. Because of the absence of bone cells, it generally needs to be combined with other graft materials.
Synthetic Bone
Synthetic bone grafts, often referred to as ceramics, are composed of calcium-based materials designed to mimic the shape and consistency of natural bone. One advantage of ceramics is that they are cadaver-free and readily available in large quantities.
However, like DBM, synthetic grafts lack bone-forming cells and proteins necessary to stimulate bone growth. Consequently, synthetic grafts must be used in combination with other bone products to achieve successful fusion outcomes.