Lunotriquetral injury is far more rare than scapholunate ligament injury.
Presentation
- History
- Distinguishing between a recent acute traumatic injury and a degenerative pathology is essential.
- Is there a history of acute trauma? What was the mechanism? Are there any other injuries (e.g. elbow/forearm)
- If nontraumatic, can the patient recall any previous historical injury?
- Patients may report ulnar sided wrist pain.
- This may be exacerbated when loading the wrist, especially in pronation i.e. gripping or using toolsStiffness or crepitus when using wrist
Examination
- Look/feel
- A wrist effusion may be present
- Move
- General assessment of hand function
- Special tests
- The “ballotment” test is done by holding the lunate and triquetrum between both thumbs and fingers and alternating between dorsal and volar translation, feeling for abnormal movement or clicking.
- Neurovascular status
- This is essential in acute traumatic cases. The motor and sensory function of the median, ulnar, and radial nerves must be assessed and documented, along with the vascular status.
Investigation
- If there is suspicion of an acute high energy injury to the wrist then the patient should be referred to the emergency department urgently.
- Bloods
- Typically not required
- Imaging
- PA radiograph of the wrist
- Examine for disruption of Gilula’s lines (fig xxx). A break in these lines may indicate an abnormality within the carpus
- Examine for the presence of carpal fractures or widening of distance between lunate and triquetrum of more than 2mm
- First line imaging modality.
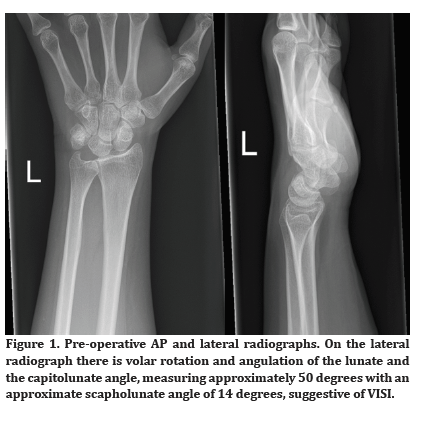
- Lateral radiograph of the wrist
- Measure the scapholunate angle, an angle <30 degrees suggests a VISI deformity
- First line imaging modality
- MRI scan
- Typically ordered from tertiary care to confirm diagnosis
Differentials
- Scapholunate ligament injury (DISI)
- Perilunate
- Perilunate dislocation or fracture dislocation
Red Flags:
Acute neurovascular deficit in an acute injury mandates emergent referralSevere diffuse swelling in a chronic setting could be an indication of underlying inflammatory arthropathy.
Management
The management depends on whether the injury is acute or chronic. All acute injuries should be referred either via the emergency department or via urgent referral to the local tertiary hand and wrist clinic.
Conservative
- Acute, undisplaced sprains can be treated with a period of immobilisation, careful clinical follow-up, and physiotherapy.
- Nonsurgical treatment is also an appropriate first line treatment in chronic degenerative situations which are minimally symptomatic in low demand patients. In these circumstances, NSAIDs when tolerated and physiotherapy are indicated.
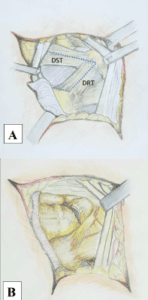
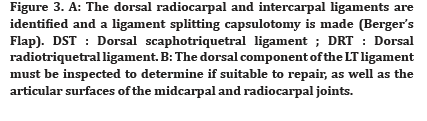
Operative
- Acute ruptures with displacement or instability, chronic but reducible ruptures, or ongoing significant pain that has failed nonsurgical treatment can be considered for surgical intervention

Prognosis/Managing Expectations
The prognosis is multifactorial and depends on the nature of the condition, the nature of the injury, and the patients functional status.