Struggling with pain at the top of your shoulder?
Distal Clavicle Osteolysis (DCO) is a treatable condition that affects the end of your collarbone at the acromioclavicular (AC) joint. Often linked to repetitive gym training or overhead sports, it can cause persistent discomfort during lifts or certain movements. With early diagnosis and structured care, full recovery is expected for most patients.
What Is Distal Clavicle Osteolysis?
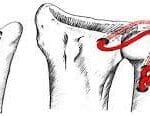
Distal Clavicle Osteolysis (DCO) occurs when the end of the collarbone (clavicle) gradually erodes where it meets the shoulder blade. This joint is known as the acromioclavicular (AC) joint. DCO leads to pain and inflammation in this area, commonly seen in people who lift weights or play sports involving repetitive overhead actions.
There are two types:
- Atraumatic DCO – develops gradually through repeated strain (e.g. bench press, overhead sports).
- Traumatic DCO – triggered by a one-off injury such as an AC-joint sprain.
Common Causes and Risk Factors
Factors that increase the risk of developing DCO include:
- Repetitive upper body load: Bench pressing, dips, push-ups, or heavy lifting
- Overhead activities: Volleyball, swimming, basketball, tennis
- Prior injuries: Especially AC-joint separation
- Intensive training: High frequency or heavy resistance (e.g. lifting >1.5 × body weight)
- Other contributors: Poor technique, fast progression in training, smoking (slows bone healing)
Typically affects active adults in their 20s and 30s, with increasing cases seen in women.
Symptoms to Look Out For
- Dull or sharp pain over the top of the shoulder (AC joint)
- Pain made worse by pressing exercises or overhead movement
- Tenderness when touching the end of the collarbone
- Discomfort when lying on the affected shoulder
- Pain at extremes of motion, especially when reaching across the body
Most people still have full range of shoulder movement.
Diagnosing Distal Clavicle Osteolysis
A healthcare professional will start with a physical examination. Diagnosis is confirmed using:
- X-rays (Zanca view): May show bone changes but often normal early on
- MRI scan: Identifies early bone damage and inflammation
- Ultrasound or bone scan: Helpful when MRI is unavailable
- Diagnostic injection: Local anaesthetic into the joint—temporary relief confirms the source
Other conditions with similar symptoms include arthritis, rotator cuff problems, or labral tears.
Treatment Options
Non-Surgical (Conservative) Care – First Line
Most patients recover well without surgery. Initial treatment includes:
- Activity adjustment: Modify pressing technique and reduce load
- Pain relief: Anti-inflammatories and ice
- Joint injection: Corticosteroids for short-term pain control
- Targeted physiotherapy:
- Phase 1: Exercises below shoulder height (e.g. wall push-ups)
- Phase 2: Progress to above shoulder level
- Phase 3: Core and shoulder stability drills
Studies show over 90% improve within 3 months of structured physiotherapy.
Surgical Treatment – If Needed
Surgery may be advised if symptoms persist despite 3 months of conservative care.
- Distal Clavicle Excision (Mumford Procedure):
- Performed via keyhole surgery (arthroscopy)
- Small portion (no more than 8 mm) of the collarbone is removed
- Recovery is quick, with return to light activity in 3 weeks and full lifting after 12 weeks
Rehabilitation mirrors non-surgical physiotherapy.
Recovery and Risks
Outlook:
- Most return to full sports or gym activity after treatment
- Long-term outcomes are excellent with proper management
Possible Complications:
- Recurrent pain if training is resumed too early
- Joint widening or early arthritis on scans
- After surgery: small risk of stiffness, infection, or bone overgrowth
Preventing DCO
- Use correct lifting technique—keep bench press grip narrower than 1.5 × shoulder width
- Increase weights gradually and take rest weeks
- Include pulling and lower body exercises to balance training
- Overhead athletes should cross-train with lower shoulder strain activities
- Avoid smoking and maintain bone health through good diet and vitamin D
Key Points for Patients
- Pain at the AC joint after lifting? DCO is a common and treatable cause
- MRI is often more useful than X-ray early on
- Adjusting your training is crucial for recovery
- Surgery is rarely needed if conservative treatment is followed properly
- A team approach leads to the best outcomes
Frequently Asked Questions
Is DCO permanent?
No. With rest and rehabilitation, bone can recover and pain usually settles within 6–12 weeks.
Can I still go to the gym?
Yes, but modify your exercises—lighter loads, shallower presses, and avoid painful positions.
Do I need an operation?
Surgery is only needed if you don’t improve after three months of structured physiotherapy.
When can I train after surgery?
Light training may start by week 3, with full return to sport around 12 weeks.
Call to Action
Still in pain at the top of your shoulder?
Request a consultation with Prof Imam’s upper-limb team today.
Visit www.TheArmDoc.co.uk or call 020 3384 5588 to schedule an appointment.
Disclaimer
This leaflet provides general information and is not a substitute for medical advice. Always speak to a qualified healthcare provider for advice specific to your condition.