Overview
Meta Description: Explore an in-depth scientific overview of Developmental Dysplasia of the Hip (DDH), its causes, risk factors, diagnosis, treatment, and long-term outcomes.
SEO Keywords: developmental dysplasia of the hip, DDH, congenital hip dislocation, infant hip dysplasia, Pavlik harness, hip surgery, orthopaedics, musculoskeletal disorders
Introduction
Developmental Dysplasia of the Hip (DDH), formerly referred to as congenital dislocation of the hip, is a complex orthopaedic condition that involves abnormal development of the hip joint. It can range from mild dysplasia, where the acetabulum is shallow, to complete dislocation. DDH affects approximately 1 in 1,000 live births and, if untreated, may lead to long-term disability.
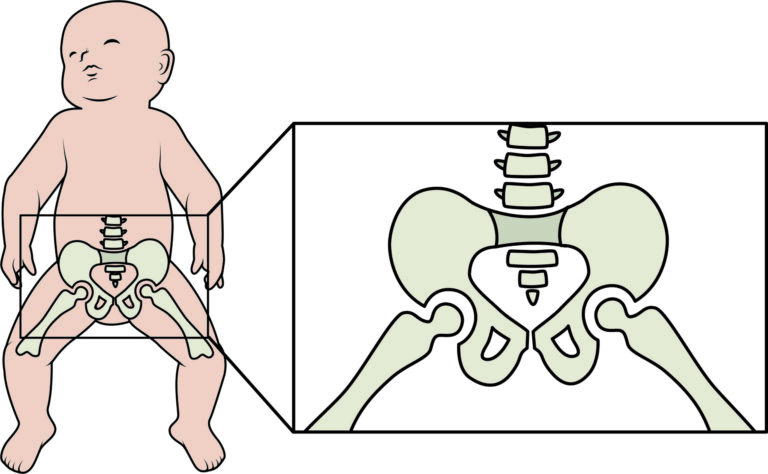
Anatomy of the Hip Joint
The hip joint is a ball-and-socket joint consisting of the femoral head (ball) and the acetabulum (socket) of the pelvis. The stability and function of the hip depend on the congruity and development of both structures. Ligaments, cartilage, and surrounding muscles provide further support.
Epidemiology of DDH
DDH has a higher prevalence in females, firstborn children, breech presentations, and in populations with traditional swaddling practices. The incidence varies globally, being higher in certain ethnic groups and geographical regions. Environmental and genetic factors play a synergistic role.
Etiology and Risk Factors
The etiology of DDH is multifactorial. Major risk factors include:
– Family history of DDH
– Female sex
– Firstborn child
– Breech position
– Oligohydramnios
– Postnatal positioning practices (tight swaddling)
Genetic predisposition contributes significantly to hip instability and improper acetabular development.
Pathophysiology
DDH develops due to the failure of normal embryological development of the hip joint. This leads to improper coverage of the femoral head by the acetabulum. Progressive changes include ligamentous laxity, shallow acetabulum, and elongation of soft tissues.
Clinical Presentation
Clinical signs vary by age:
In Newborns:
– Positive Ortolani and Barlow maneuvers
– Asymmetrical thigh folds
– Limited hip abduction
In Infants:
– Leg length discrepancy
– Limited range of motion
In Older Children:
– Limping
– Trendelenburg gait
– Hip pain
In Adolescents and Adults:
– Early onset osteoarthritis
– Hip instability and chronic pain
Diagnosis
Timely diagnosis is critical for effective treatment. Diagnostic methods include:
– Clinical physical examination (Ortolani and Barlow tests)
– Ultrasonography (especially before 6 months of age)
– Radiographs (after ossification of the femoral head)
– MRI or CT scans in complex or postoperative cases
Classification Systems
Several classification systems are used to describe the severity of DDH:
– Graf Ultrasound Classification
– Tönnis Classification
– International Hip Dysplasia Institute (IHDI) Classification
Management Strategies by Age
Treatment depends on the age and severity of DDH:
0–6 Months:
– Pavlik harness to maintain femoral head position
6–18 Months:
– Closed reduction under anesthesia
– Hip spica cast
18 Months – 2 Years:
– Open reduction surgery
Above 2 Years:
– Open reduction with osteotomy (Salter, Dega, Pemberton)
– Femoral shortening if necessary
Surgical Techniques
Surgical interventions vary based on the patient’s age and hip morphology:
– Open Reduction
– Salter Innominate Osteotomy
– Pemberton Osteotomy
– Dega Osteotomy
– Femoral Osteotomy
Postoperative immobilization and physiotherapy are essential for recovery.
Complications of DDH Treatment
Potential complications include:
– Avascular necrosis (AVN) of the femoral head
– Redislocation or subluxation
– Leg length discrepancy
– Joint stiffness
– Premature arthritis
Rehabilitation and Follow-Up Care
Rehabilitation includes:
– Gradual weight bearing
– Physiotherapy for muscle strengthening
– Serial imaging to monitor growth
Follow-up is essential until skeletal maturity to identify recurrence or late complications.
Long-Term Outcomes
When treated early, most children achieve normal hip function. Delayed diagnosis or inadequate treatment increases the risk of long-term sequelae, including chronic pain, gait abnormalities, and early arthritis.
Psychosocial and Quality of Life Considerations
Children and families may face challenges including limited mobility, psychological stress, and social isolation. Comprehensive care should include psychosocial support and parental education.
Preventive Strategies
Preventive measures include:
– Universal hip screening at birth
– Parental education about safe swaddling
– Early referral to orthopaedic specialists for high-risk infants
Research and Advances in DDH
Ongoing research focuses on:
– Genetic markers
– Improved imaging modalities
– Minimally invasive surgical techniques
– Long-term functional outcomes monitoring
Conclusion
Developmental Dysplasia of the Hip is a significant paediatric orthopaedic condition with lifelong implications if untreated. Timely diagnosis, individualized treatment, and long-term follow-up are essential to achieving