Overview:
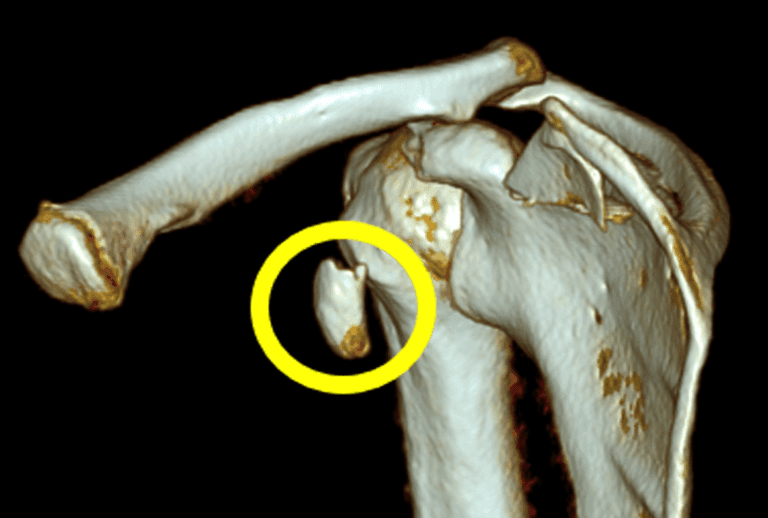
Coracoid fractures are rare injuries often associated with other shoulder injuries like AC joint dislocations or fractures of the scapula, clavicle, and humerus.
What is the Coracoid Process?
The coracoid process is a small bony projection on the scapula (shoulder blade).
Causes of Coracoid Fractures:
- Direct Trauma: Such as a direct blow to the shoulder.
- Repetitive Stress: Overuse injuries from activities like throwing or lifting.

Symptoms:
- Pain: Severe pain around the coracoid process.
- Tenderness: Pain when touching the area.
- Limited Movement: Difficulty moving the arm.
Diagnosing Coracoid Fractures:
- Physical Examination: Checking for pain, tenderness, and limited movement.
- Imaging:
- X-rays: Standard views to see the fracture.
- CT Scans: For detailed images.
- MRI: Useful for assessing ligament injuries around the coracoid.
Types of Fractures:
- Ogawa Classification: Divides fractures based on their location relative to the coracoclavicular ligament.
- Type I: Fracture behind the ligament, often needing surgery.
- Type II: Fracture in front of the ligament, usually managed without surgery.
- Eyres Classification: Categorizes fractures into five types based on their location and extent.

Treatment Options:
- Non-Surgical Management:
- Suitable for isolated and minimally displaced fractures.
- Immobilization: Using a sling for four weeks.
- Rehabilitation: Gradual exercises to restore movement and strength.
- Surgical Management:
- Needed for significantly displaced fractures or those associated with other shoulder injuries.
- Surgical Techniques: Various approaches to fix the fracture using screws or plates.

Post-Operative Rehabilitation:
- Initial Immobilization: Using a sling.
- Gradual Exercises: Starting with passive movements and progressing to active and strengthening exercises.
- Full Recovery: Typically within 2-3 months.
Possible Complications:
- Non-Union: Bone fails to heal.
- Persistent Pain: May require hardware removal.
- Limited Movement: Ensuring full range of motion through rehabilitation.
Lessons Learned:
- Accurate diagnosis and imaging are essential.
- Non-surgical treatment works for most isolated, minimally displaced fractures.
- Surgery is necessary for significantly displaced fractures or those associated with other shoulder injuries.
- Detailed pre-operative planning and proper surgical techniques are crucial for optimal outcomes.
- Individualized treatment plans based on the fracture and patient factors lead to the best outcomes.