Understanding Avascular Necrosis: Causes, Effects, and Treatment Options
Osteonecrosis of the hip occurs when the blood supply to the femoral head is disrupted. Without sufficient blood flow, the bone tissue in the femoral head deteriorates and collapses over time
Published
13 November 2024
Reading time
8 min
Words
1,861
Sections
4
Osteonecrosis of the hip, also known as avascular necrosis (AVN) or aseptic necrosis, is a debilitating condition caused by a disruption in the blood supply to the femoral head (thighbone). Without adequate blood flow, bone cells cannot survive, leading to the gradual breakdown of the hip joint and, over time, severe arthritis.
Although avascular necrosis can affect any bone, the hip is the most commonly impacted site. Each year, over 20,000 individuals require hospitalization for treatment, with many cases involving both hips. Early diagnosis and timely intervention are essential to manage this painful condition and prevent joint degeneration.
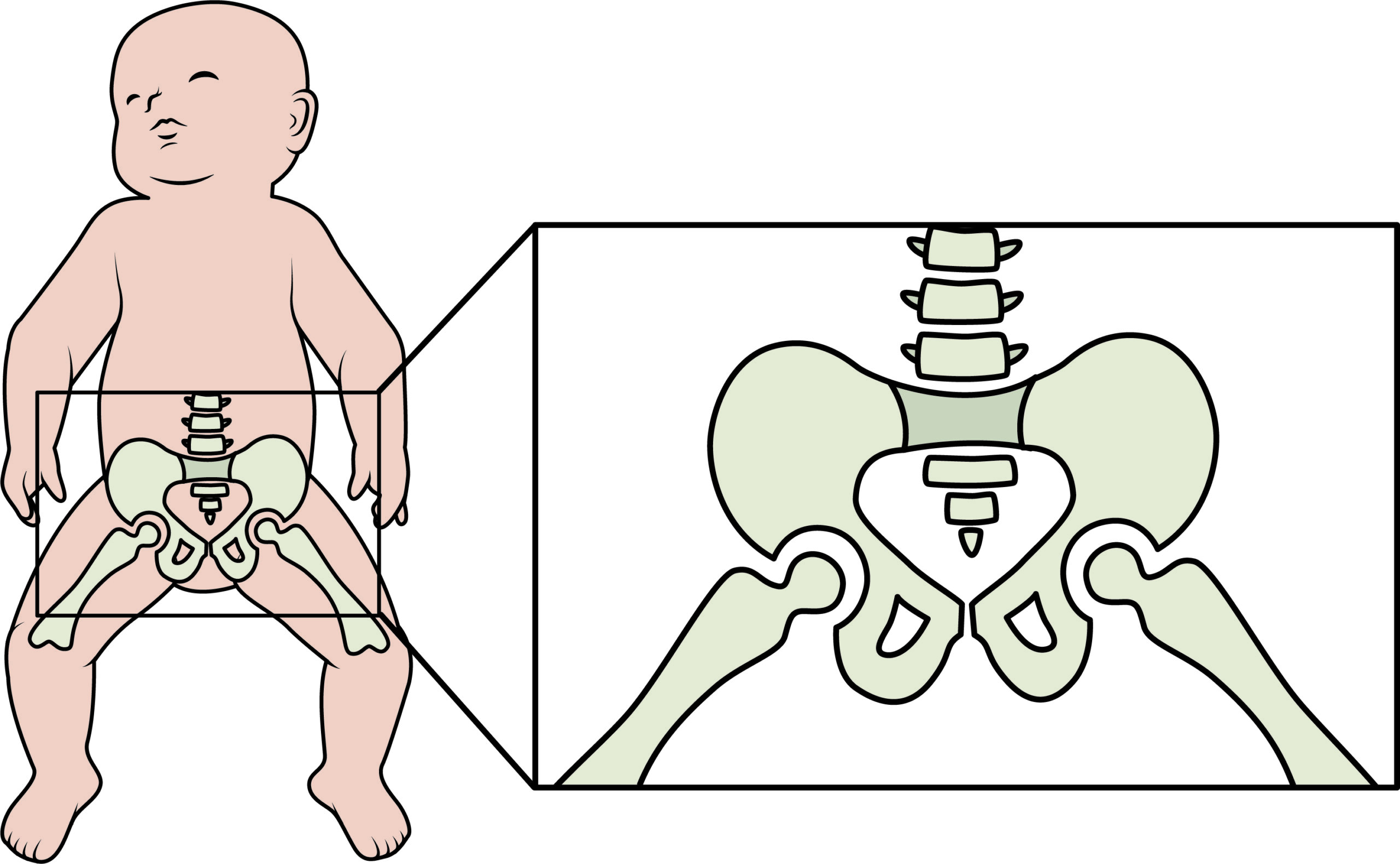
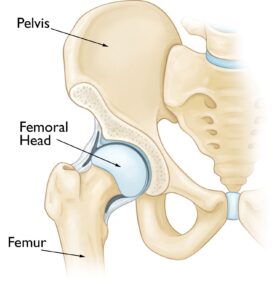
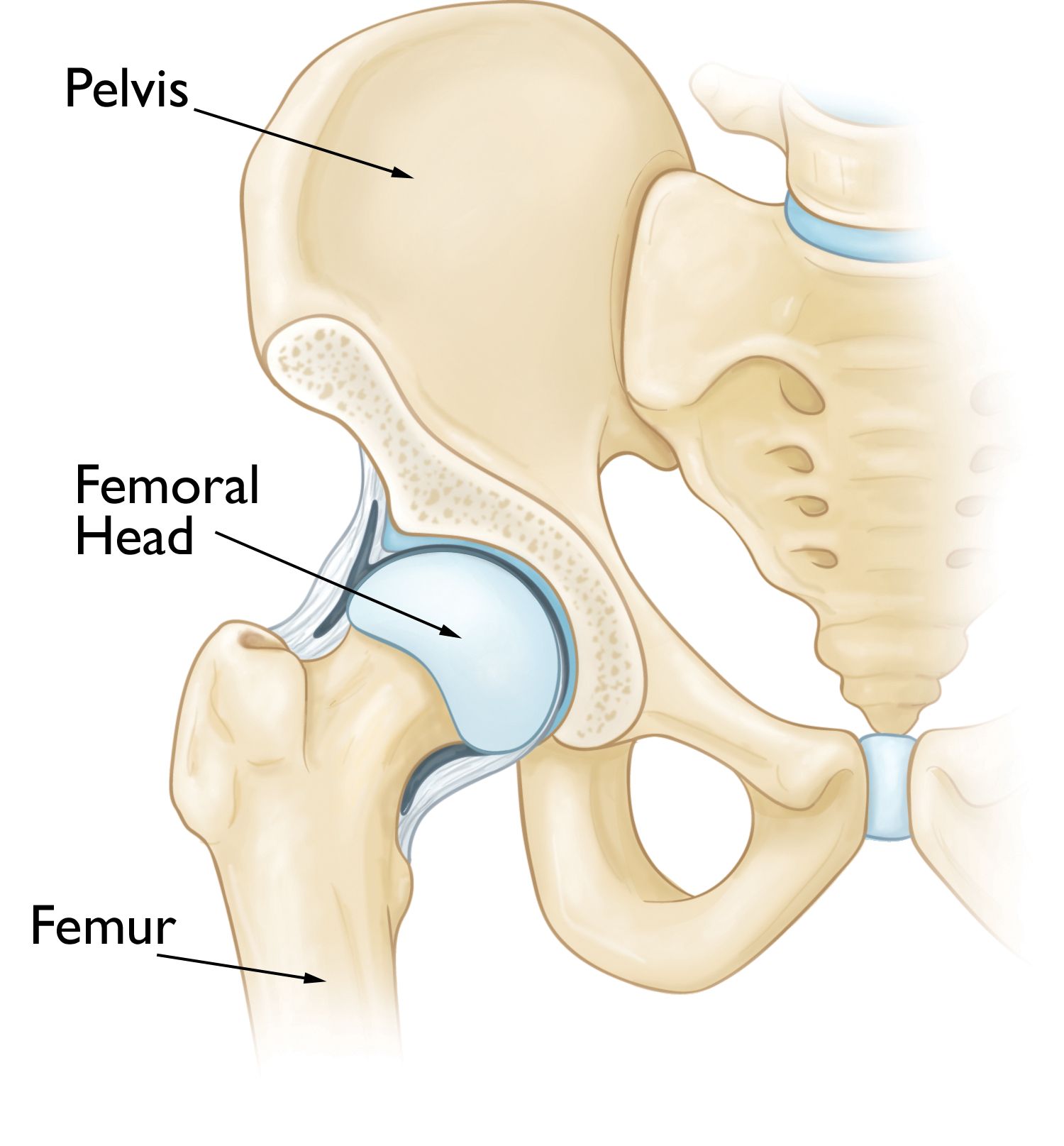
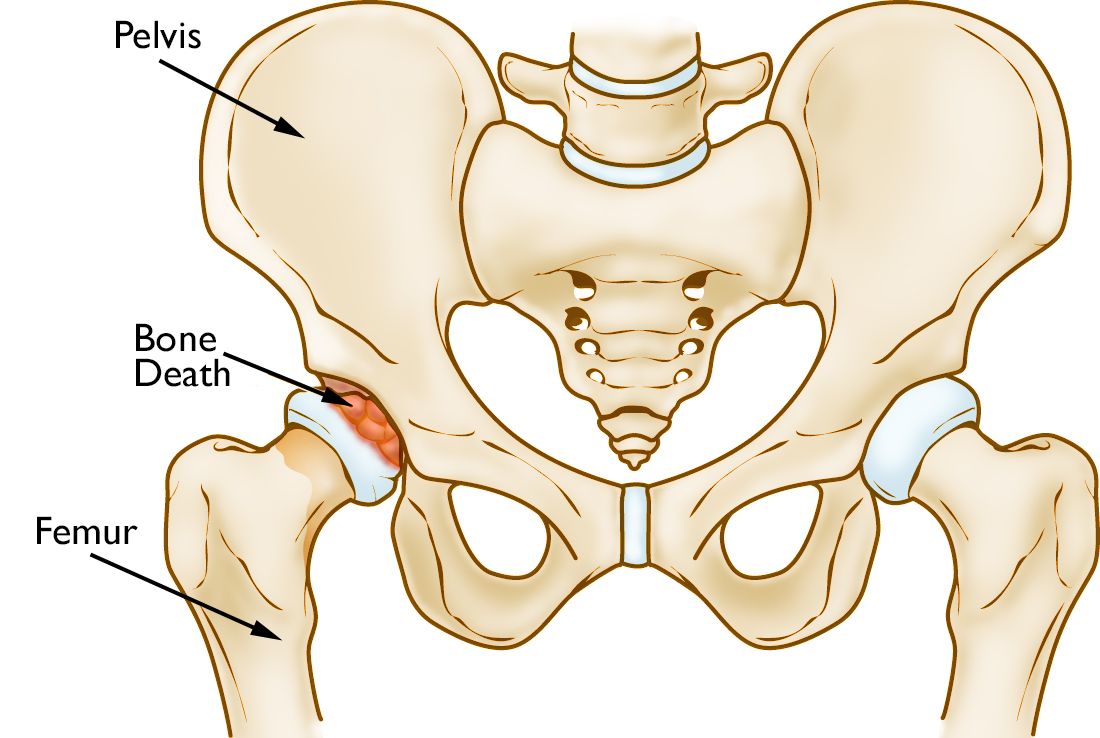
Anatomy
The hip joint functions as a ball-and-socket mechanism, allowing a wide range of motion.
The socket, known as the acetabulum, is part of the pelvis.
The ball is the femoral head, located at the upper end of the femur (thighbone).
Both the ball and socket are coated with a layer of articular cartilage, a smooth and slippery tissue that cushions the bones and facilitates seamless movement within the joint.
Osteonecrosis of the hip occurs in the femoral head, which is the ball of ball-and-socket hip joint.
Causes
Osteonecrosis of the hip occurs when the blood supply to the femoral head is disrupted. Without sufficient blood flow, the bone tissue in the femoral head deteriorates and collapses over time. This also leads to the collapse of the articular cartilage covering the joint, resulting in severe arthritis and impaired mobility.
This condition can affect individuals of any age but is most prevalent among those aged 40 to 65. Men are more frequently diagnosed with osteonecrosis of the hip than women.
Risk Factors
While the precise cause of disrupted blood flow is not always clear, several risk factors have been linked to the development of osteonecrosis:
Injuries: Trauma such as hip dislocations, fractures, or other injuries can damage blood vessels, restricting blood supply to the femoral head.
Excessive alcohol consumption: Prolonged heavy drinking can lead to the formation of fatty deposits in blood vessels, reducing blood flow to bone tissue and increasing cortisone levels, which may contribute to osteonecrosis.
Corticosteroid use: Long-term use of corticosteroid medications, often prescribed for conditions like asthma, rheumatoid arthritis, and lupus, is associated with an increased risk of osteonecrosis. While the exact mechanism is unclear, studies suggest a significant correlation.
Underlying medical conditions: Osteonecrosis has been linked to several diseases, including:
Caisson disease (decompression sickness or "the bends")
Sickle cell disease
Myeloproliferative disorders
Gaucher's disease
Systemic lupus erythematosus
Crohn's disease
Arterial embolism or thrombosis
Vasculitis
Awareness of these risk factors can aid in early diagnosis and intervention, reducing the likelihood of severe joint damage.
In osteonecrosis, the bone in the head of the femur slowly dies.
Symptoms
Osteonecrosis progresses through distinct stages, with hip pain often being the initial symptom. This discomfort may begin as a dull ache or a persistent throbbing sensation in the groin or buttock area.
As the condition advances, pain intensifies, making it increasingly difficult to bear weight on the affected hip. Movement of the hip joint becomes progressively painful, significantly affecting mobility and quality of life.
The progression of osteonecrosis can span several months to over a year. Early diagnosis is crucial, as research suggests that timely intervention can lead to more favorable outcomes, potentially slowing the disease's advancement and preserving joint function.
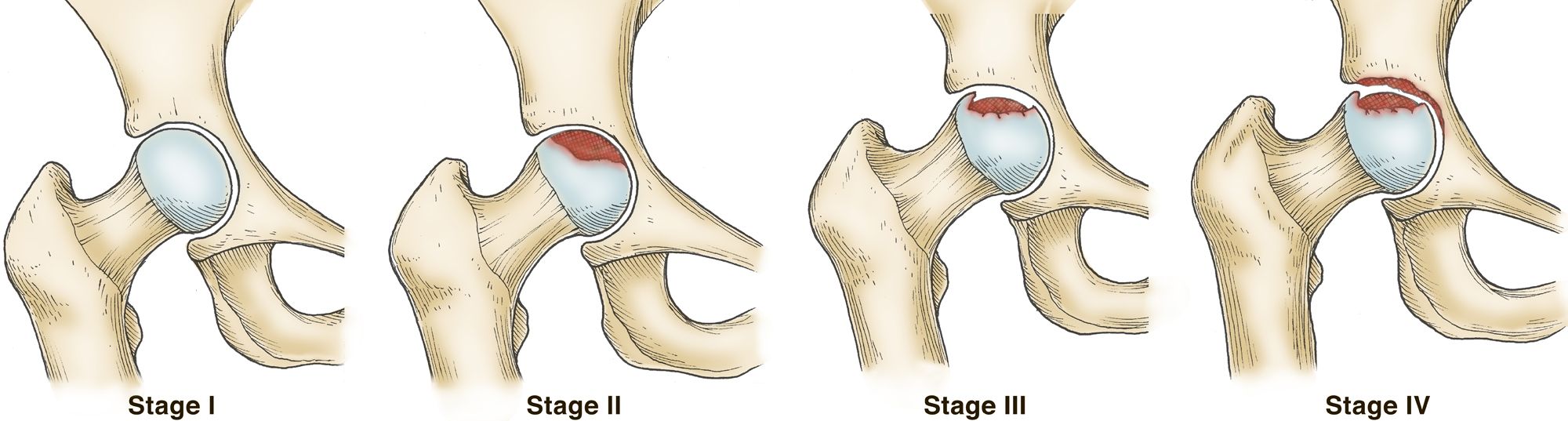
The four stages of osteonecrosis. The disease can progress from a normal, healthy hip (Stage I) to the collapse of the femoral head and severe osteoarthritis (Stage IV).''
Doctor Examination
During your medical visit, the doctor will begin by discussing your symptoms and reviewing your medical history. A physical examination of the hip will follow, focusing on identifying specific movements that trigger pain.
In the early stages of osteonecrosis, patients often experience significant pain in the hip joint while maintaining relatively good range of motion. This is because, initially, only the femoral head is affected. However, as the disease progresses and the femoral head collapses, the joint surface deteriorates, leading to arthritis. At this stage, stiffness and loss of motion become more apparent, further impairing mobility. Early detection during the examination is vital for effective management of the condition.
During the exam, the doctor will move your hip in different ways to learn more about your pain.'
Imaging Tests
Imaging tests are essential for confirming the diagnosis of osteonecrosis and assessing the extent of damage to the hip joint.
X-rays: X-rays are commonly used to capture detailed images of dense structures like bones. They help determine whether the femoral head has collapsed and assess the severity of the condition. X-rays are particularly effective in identifying structural changes in advanced stages of osteonecrosis.
These imaging studies provide critical information, guiding the doctor in selecting the most appropriate treatment plan for your condition.
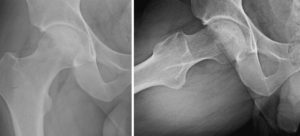
(Left) An X-ray of a healthy hip joint. (Right)' In this X-ray, the osteonecrosis has progressed to collapse of the femoral head.
Imaging Findings in Osteonecrosis
In osteonecrosis, the affected area of the femoral head typically appears as a wedge-shaped region with a distinct, dense whitish sclerotic (hardened) border. This is most commonly observed in the superior lateral portion of the femoral head.
On a lateral X-ray view, a characteristic feature called the 'crescent sign' may be visible just beneath the surface of the femoral head. This line represents the collapse of subchondral bone and is a key indicator of osteonecrosis in its progressive stages. Identifying these imaging markers is crucial for accurate diagnosis and treatment planning.
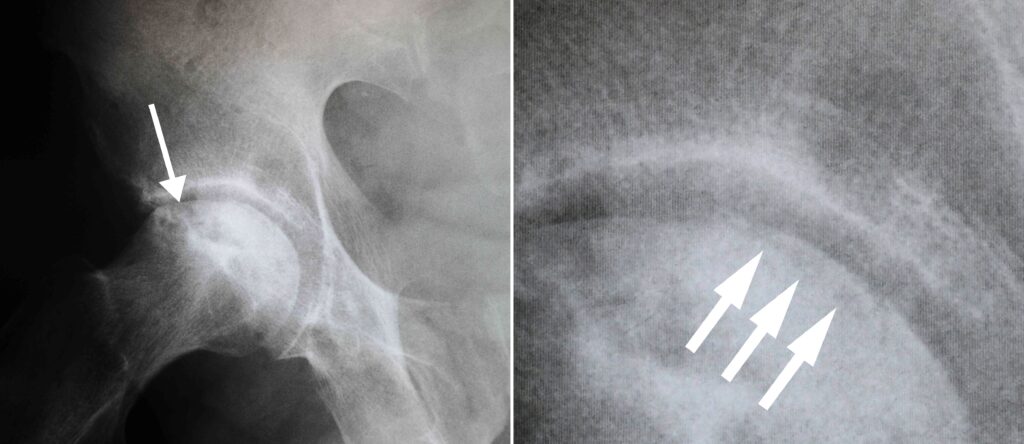
(Left)'This X-ray shows osteonecrosis of the hip.'(Right)'When viewed close up, the X-ray reveals the 'crescent sign' that is typically seen before collapse of the femoral head.'
Imaging Findings in Osteonecrosis
In osteonecrosis, the affected area of the femoral head typically appears as a wedge-shaped region with a distinct, dense whitish sclerotic (hardened) border. This is most commonly observed in the superior lateral portion of the femoral head.
On a lateral X-ray view, a characteristic feature called the 'crescent sign' may be visible just beneath the surface of the femoral head. This line represents the collapse of subchondral bone and is a key indicator of osteonecrosis in its progressive stages. Identifying these imaging markers is crucial for accurate diagnosis and treatment planning.
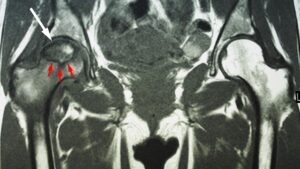
This MRI scan shows osteonecrosis in a patient's right hip (white arrow). The dark line (red arrows) denotes the border between dead bone and living bone. The patient's left hip is normal.
Treatment Options for Osteonecrosis of the Hip
While nonsurgical treatments'such as anti-inflammatory medications, activity modifications, and the use of crutches'can help alleviate pain and slow disease progression, surgical procedures are typically the most effective approach for managing osteonecrosis. Early-stage osteonecrosis, before the femoral head collapses, offers the best opportunity for hip-preserving treatments.
Core Decompression and Grafting
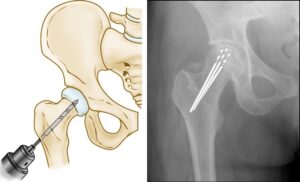
Core decompression is a surgical technique used to alleviate pressure within the femoral head. The procedure involves drilling one large or several small holes into the bone to:
Relieve internal pressure.
Promote the formation of new blood vessels to reestablish nourishment to the affected bone tissue.
When performed in the early stages of osteonecrosis, core decompression can often prevent the collapse of the femoral head and reduce the likelihood of arthritis developing in the hip. This procedure is particularly effective when the disease is detected before significant joint damage occurs.
(Left) Illustration of core decompression. (Right) In this X-ray, the drill lines show the pathway of the small drill holes used in the procedure.'
Advanced Surgical Techniques for Osteonecrosis of the Hip
In many cases, core decompression is combined with bone and cartilage grafting to encourage the regeneration of healthy bone tissue and support cartilage in the hip joint. A bone graft involves transplanting healthy bone tissue to the affected area. This tissue can be sourced from:
A donor (allograft), or
Your own body (autograft), typically from another bone.
Modern advancements have also introduced synthetic bone grafts, which may be mixed with a patient's own bone marrow cells to enhance the regeneration process. Discussing the available grafting options with your surgeon is crucial to determine the best approach for your specific condition.
Vascularized Fibula Graft
Another effective surgical option is the vascularized fibula graft. In this procedure:
A section of bone is harvested from the fibula (the smaller bone in your leg), along with its attached blood supply, including an artery and a vein.
The graft is then transplanted into a channel created in the femoral neck and head.
The artery and vein from the graft are reconnected to restore blood flow, promoting healing and revitalization of the osteonecrotic area.
This procedure is particularly beneficial in cases where core decompression alone may not be sufficient, offering a robust solution to preserve hip function and prevent further deterioration.
Two different X-ray views showing osteonecrosis of the hip.
Two different X-ray views showing osteonecrosis of the hip.
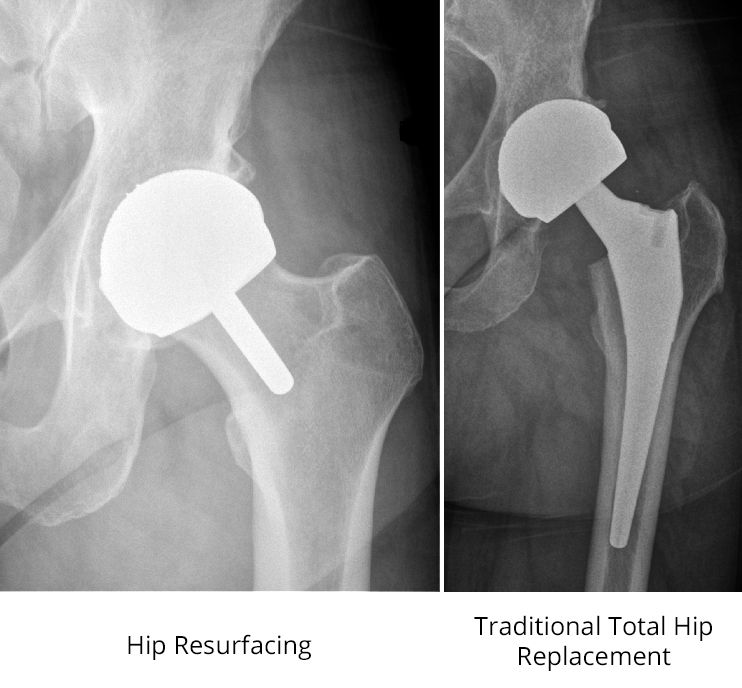
Total Hip Replacement: A Definitive Solution for Advanced Osteonecrosis
When osteonecrosis progresses to the stage where the femoral head has collapsed, total hip replacement (THR) becomes the most effective treatment option.
This surgical procedure involves:
Removing the damaged bone and cartilage from the hip joint.
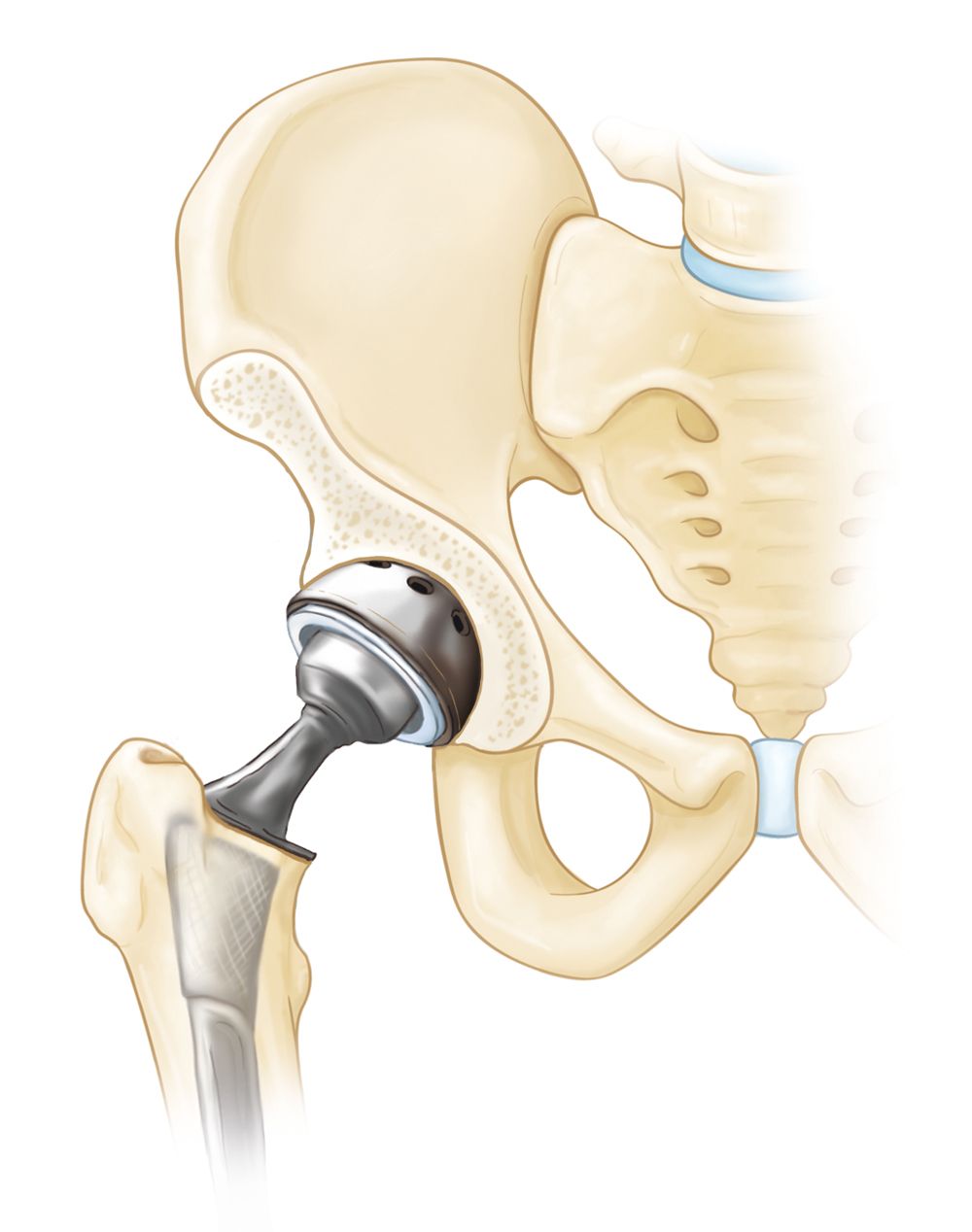
Replacing the joint surfaces with prosthetic components made of durable materials, such as metal or plastic.
Total hip replacement not only alleviates pain but also restores the function and mobility of the hip, significantly improving the patient's quality of life. This approach is particularly successful for individuals with severe joint damage who have not responded to other treatments.
In total hip replacement, both the head of the femur and the socket are replaced with an artificial device.
Expected Outcomes of Osteonecrosis Treatments
The success of treatment for osteonecrosis largely depends on the stage of the disease at the time of diagnosis and intervention.
Core Decompression
Effectiveness: Core decompression can prevent osteonecrosis from advancing to severe arthritis and the need for total hip replacement, especially when performed in the early stages before bone collapse.
Healing Process: In successful cases, the bone regains its blood supply, and healing occurs over several months. During this time, patients must use crutches or a walker to minimize stress on the affected hip.
Recovery Timeline: Most patients return to walking without assistance within three months and experience significant pain relief.
Vascularized Fibular Grafting
Procedure and Healing: This invasive technique requires a longer recovery period. Patients typically remain non-weightbearing for several weeks before gradually resuming weightbearing with the help of a walker or cane.
Outcome: When performed before femoral head collapse, vascularized fibular grafting yields favorable results, promoting healing and preserving joint function.
Total Hip Replacement
When Necessary: If osteonecrosis is diagnosed after the femoral head has collapsed, core decompression is unlikely to be effective. In these cases, a total hip replacement is the preferred treatment.
Results: Total hip replacement reliably alleviates pain and restores hip function, offering excellent outcomes for most patients with advanced osteonecrosis.
Conclusion
Early diagnosis and treatment are critical in determining the success of these procedures. While core decompression and vascularized fibular grafting are effective in early-stage cases, total hip replacement remains the gold standard for managing advanced osteonecrosis.
Every article on OrthoGlobe is reviewed by practising orthopaedic surgeons for clinical accuracy and plain-language clarity. Content is for education only and does not replace advice from your treating clinician.
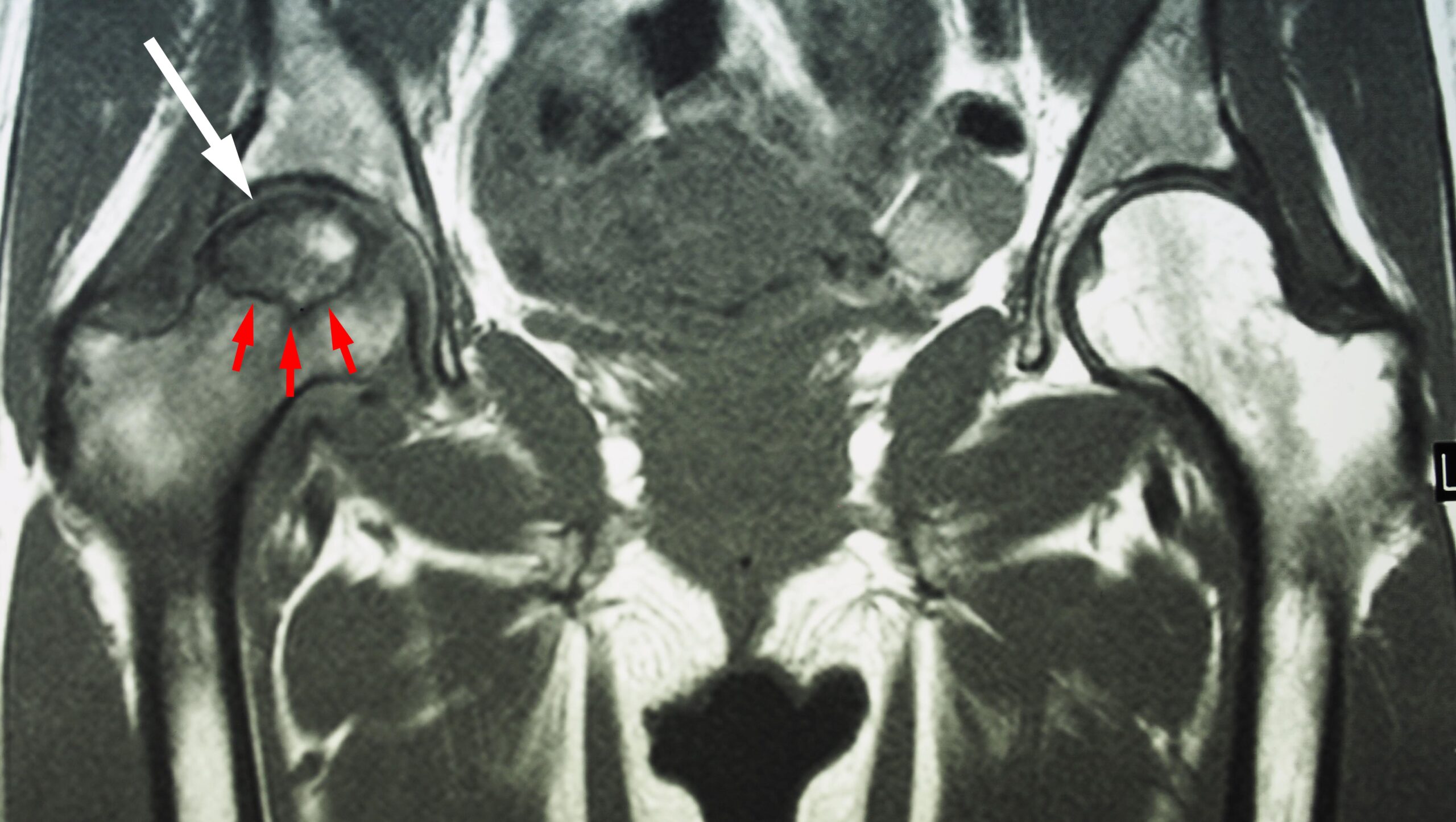


 This MRI scan shows osteonecrosis in a patient's right hip (white arrow). The dark line (red arrows) denotes the border between dead bone and living bone. The patient's left hip is normal.
This MRI scan shows osteonecrosis in a patient's right hip (white arrow). The dark line (red arrows) denotes the border between dead bone and living bone. The patient's left hip is normal.