 2
2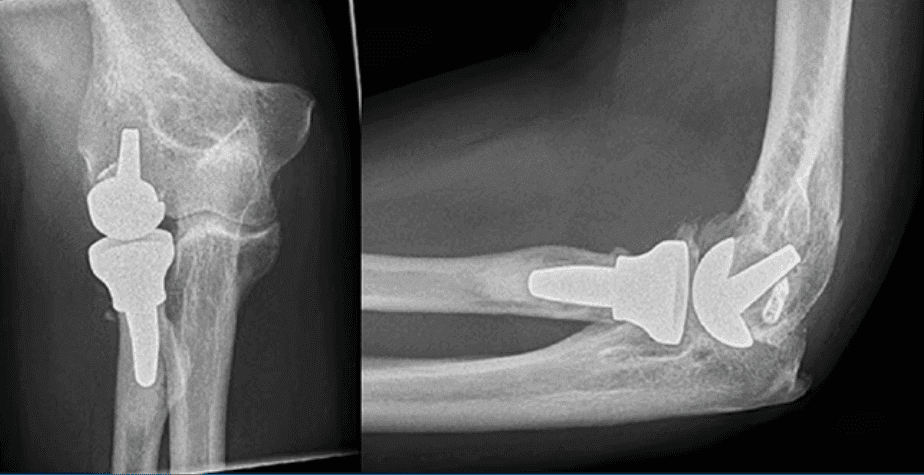 3
3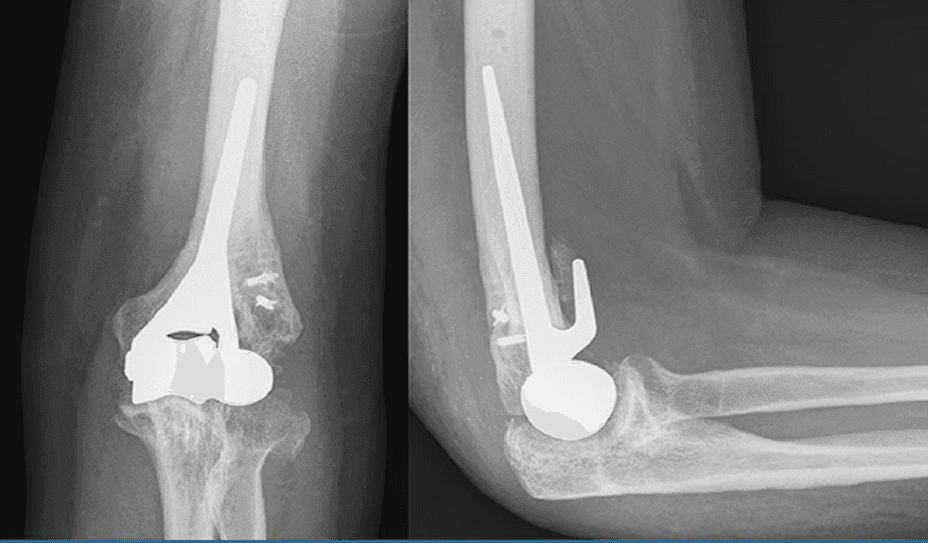 4
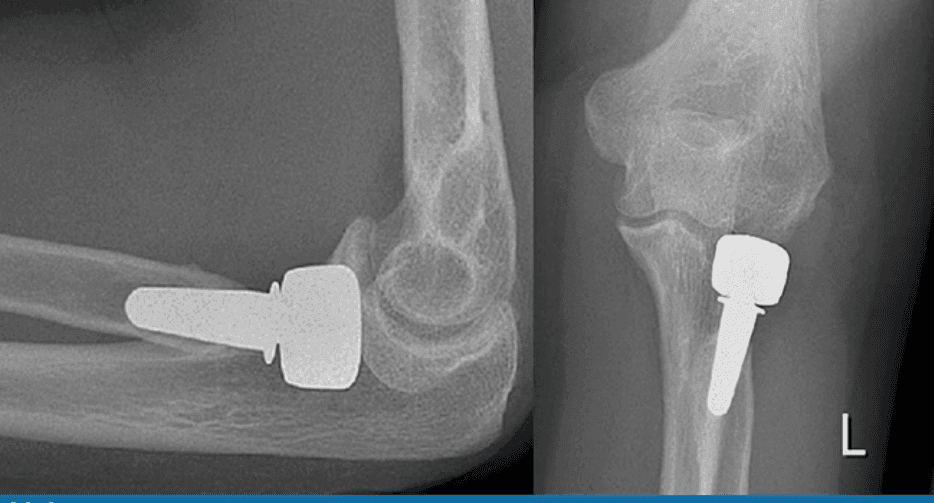
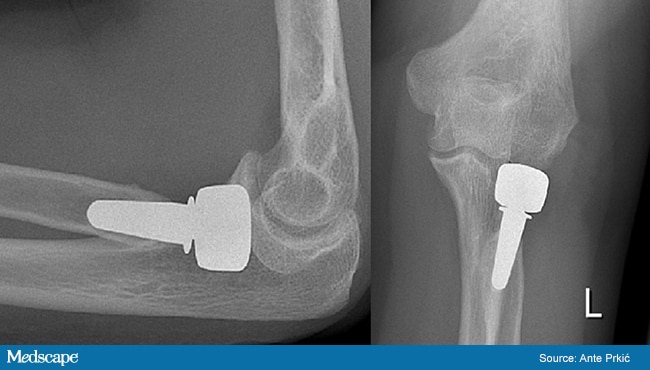
4Furthermore, possible implant-specific long-term complications influence decision-making on the part of the surgeon. Radial head prostheses may lead to excessive wear of and pain in the capitellum.[8]'Hemiarthroplasty does not replace the ulna and radius, which may lead to painful degeneration of these native articulating surfaces.[9]'Unicompartmental arthroplasty relieves only pronation/supination problems, and has only a slight effect on flexion/extension.
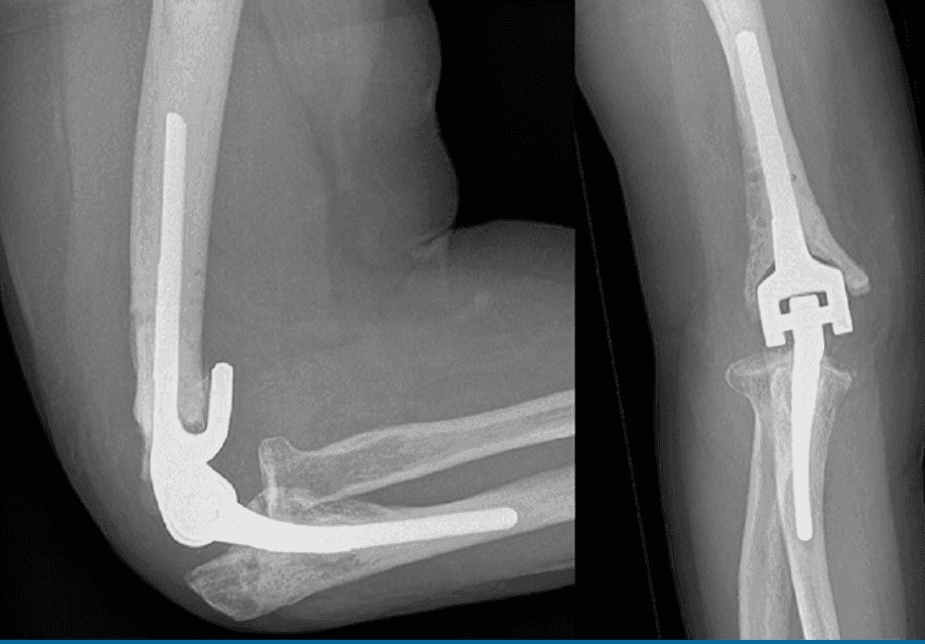
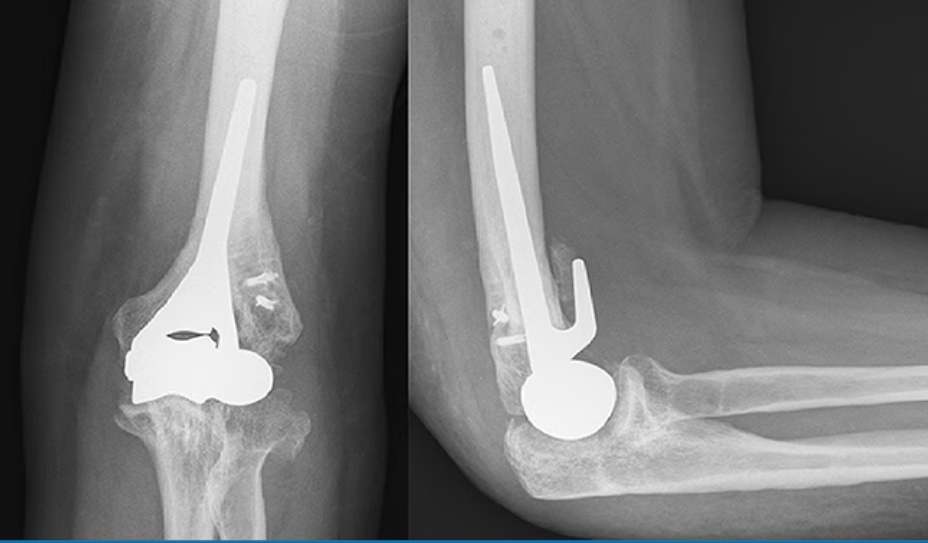
In total elbow arthroplasty, two main models are currently available: linked and unlinked designs. Linked (or semi-) constrained elbows have a mechanical connection between the humeral and ulnar components that prevents disassociation. These implants do not rely on muscular or ligamentous tissues for stability.
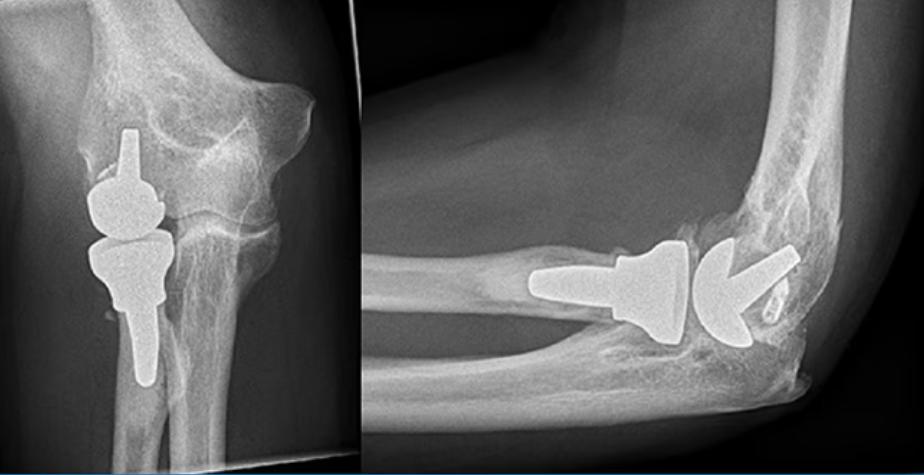
Unlinked implants have no physical connection between the humeral and ulnar components. They rely on bearing surface architecture as well as soft-tissue integrity for elbow stability.
Unlinked total elbow arthroplasty consists of two separate implants and relies more on ligamentous stability, as opposed to linked arthroplasties, which have more intrinsic stability. This difference implies that unlinked arthroplasties are less suitable in patients with severe ligamentous instability, as seen in long-standing rheumatoid arthritis, because of a high dislocation rate. In these cases, the use of linked designs is advisable.
'In one modern design'the latitude total elbow arthroplasty'it is possible to decide during surgery whether to use a linked or unlinked version of the implant because this prosthesis offers an optional part for constrainment of the hinge.
The inherent stability of the linked designs may result in higher forces being transferred across the implant/cement and cement/bone interfaces. This is why modern designs use a 'sloppy' hinge, having 7'-10'0'varus/valgus inherent laxity at the hinge section, with a minimal motion-bearing contact area; this aims to maintain intrinsic stability without the risk for early loosening.
The fixation technique may be cemented or uncemented, with a bone-ingrowth coating. Cemented designs have the advantage of instant fixation, which might be favorable in the linked designs regarding the previously mentioned pulling-out forces. However, a long cement mantle may result in elaborate surgery if revision is necessary.
Considerations for Periprocedural Care
Regarding the affected joint and patient symptoms, pain relief and/or enhancement of range of motion should be pursued, depending on the patient's expectations and wishes. It is also necessary to inform patients that even though a joint is replaced, it can never reach the level of a healthy native joint. Therefore, activities should be adapted, and high-impact forces avoided, to decrease the chance of the implant loosening or of periprosthetic fractures. For example, patients with a total elbow arthroplasty are advised not to lift more than 5 kg at once, although this is based on empirical experience; no trials on use and the impact of use on implant survival have been published.
Triceps-On and Triceps-Off Techniques
To achieve good intra-articular exposure, two approach techniques can be distinguished: triceps-on and triceps-off. The triceps-on technique without olecranon osteotomy leaves the patient with a larger range of motion postoperatively, with no additional complications, even though the surgical exposure of the operative field is technically more challenging. The triceps-on Bryan-Morrey approach is performed by making a window medial to the distal triceps tendon.A variant to this approach uses windows on both sides of the triceps.Another triceps-sparing approach is to perform a chevron osteotomy and to reattach the osseous insertion of the triceps afterwards.'Triceps-off approaches use subperiostal dissection of the triceps insertion and refixation using tension band wiring. It is also possible to dissect the triceps muscle longitudinally along the muscle fibers and to approach the elbow joint posteriorly.
Ideally, triceps function is protected as much as possible to aid in postoperative rehabilitation and prevention of a flexion contracture.
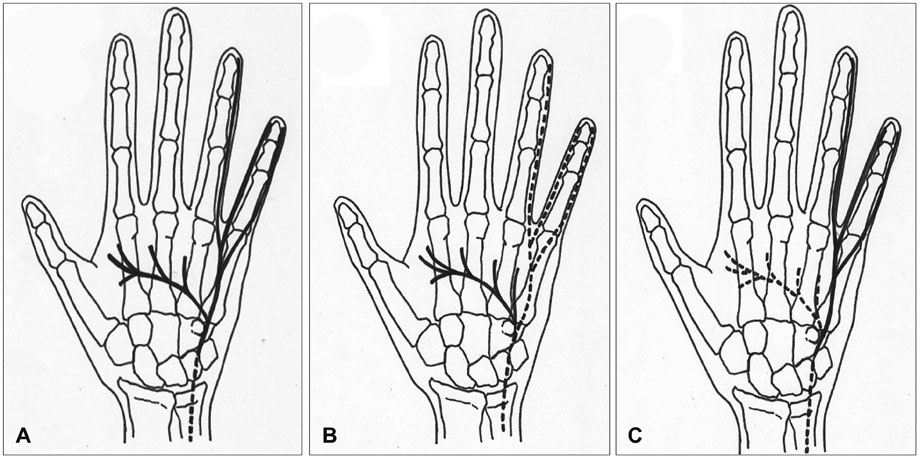
Third, the Boyd approach uses the ulnar insertion of the anconeus and supinator muscles as an en bloc flap, which protects the PIN.However, the dorsal recurrent artery is at risk to be damaged during reflection of the muscles.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}